Вам также может понравиться
- Abstract PRF and ApplicationДокумент1 страницаAbstract PRF and Applicationkuncupcupu1368Оценок пока нет
- CHOLEDOCHOLITHIASISДокумент8 страницCHOLEDOCHOLITHIASISkuncupcupu1368Оценок пока нет
- Physiology & Pathophysiology of PainДокумент31 страницаPhysiology & Pathophysiology of Painkuncupcupu1368Оценок пока нет
- Cystostomy NewДокумент32 страницыCystostomy Newkuncupcupu1368Оценок пока нет
- Candida ScoreДокумент7 страницCandida ScoreRaditya Indah TofaniОценок пока нет
- Hemodialysis: Indication: Volume Overload Acidosis (PH 6.5) UremiaДокумент9 страницHemodialysis: Indication: Volume Overload Acidosis (PH 6.5) Uremiakuncupcupu1368Оценок пока нет
- Beta Blocker AgentsДокумент28 страницBeta Blocker Agentskuncupcupu1368Оценок пока нет
- Acute Cor PulmonaleДокумент25 страницAcute Cor Pulmonalekuncupcupu1368Оценок пока нет
- Regulation of Cell Division: AP BiologyДокумент25 страницRegulation of Cell Division: AP Biologykuncupcupu1368Оценок пока нет
- MR 2 Julii 2013Документ15 страницMR 2 Julii 2013kuncupcupu1368Оценок пока нет
- Hypoglycemia, Hyperosmolar Hyperglycaemic State (HHS) and Diabetic Ketoacidosis (Dka)Документ30 страницHypoglycemia, Hyperosmolar Hyperglycaemic State (HHS) and Diabetic Ketoacidosis (Dka)kuncupcupu1368Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- F Ac 18 1 2012 0510Документ36 страницF Ac 18 1 2012 0510Handugan Quinlog NoelОценок пока нет
- Sebiomo Et AlДокумент5 страницSebiomo Et AlAnkit VermaОценок пока нет
- FDA与ISPE关于质量量度的试点计划Документ14 страницFDA与ISPE关于质量量度的试点计划windli2014Оценок пока нет
- Desired Characteristics and Applications of SuspensionsДокумент8 страницDesired Characteristics and Applications of Suspensionsasad bashirОценок пока нет
- Drugs Tema Proiect Engleza 2Документ1 страницаDrugs Tema Proiect Engleza 2ClaudiuDragomirОценок пока нет
- Antineoplastic Agents ReportДокумент3 страницыAntineoplastic Agents ReportMegan Rose MontillaОценок пока нет
- Study On Demonetization and Its Impact On The Automobile SectorДокумент5 страницStudy On Demonetization and Its Impact On The Automobile SectorVinayak DesaiОценок пока нет
- Drug StudyДокумент34 страницыDrug Studypoleene de leonОценок пока нет
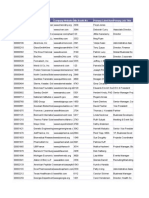
- PCP Network List Oct.02Документ96 страницPCP Network List Oct.02ashrookpОценок пока нет
- MicrobiologyДокумент688 страницMicrobiologyeko1980100% (1)
- Medicinal Application PDFДокумент11 страницMedicinal Application PDFrishabh singhОценок пока нет
- Master Class Invitation LetterДокумент3 страницыMaster Class Invitation LetterJamil B. AsumОценок пока нет
- Drug Study 408Документ13 страницDrug Study 408Jheryck SabadaoОценок пока нет
- Barriers For Pharmaceutical Innovation With Focus in Cancer Drugs, The Case of MexicoДокумент11 страницBarriers For Pharmaceutical Innovation With Focus in Cancer Drugs, The Case of MexicoLiz SernaОценок пока нет
- Formulation Flexibility Broadens The Oral Thin Film - Oral Drug Delivery May 2011Документ3 страницыFormulation Flexibility Broadens The Oral Thin Film - Oral Drug Delivery May 2011Reza-ul JalilОценок пока нет
- Exhibitor List 10-23-09 - Pharma CosДокумент28 страницExhibitor List 10-23-09 - Pharma CosKristineCostanzaОценок пока нет
- Chronic Pain Management ChartsДокумент2 страницыChronic Pain Management Chartslrpokhrel100% (3)
- Development and Validation of Quantitative Determination and Sampling Methods For Acetaminophen Residues On Pharmaceutical Equipment SurfacesДокумент7 страницDevelopment and Validation of Quantitative Determination and Sampling Methods For Acetaminophen Residues On Pharmaceutical Equipment SurfacesDItaОценок пока нет
- Chapter 4 PDFДокумент24 страницыChapter 4 PDFMd. Badrul IslamОценок пока нет
- Nifedipine+for+preterm+labour PPG v4 1 PDFДокумент9 страницNifedipine+for+preterm+labour PPG v4 1 PDFosezele emekaОценок пока нет
- Application For The POst of M.RДокумент1 страницаApplication For The POst of M.RMohammed AaquibОценок пока нет
- Single-Dose and Multiple-Dose Pharmacokinetics of Zaltoprofen After Oral Administration in Healthy Chinese VolunteersДокумент7 страницSingle-Dose and Multiple-Dose Pharmacokinetics of Zaltoprofen After Oral Administration in Healthy Chinese VolunteersSonia BaruaОценок пока нет
- Clinical Research Organization / Contract Research OrganizationДокумент34 страницыClinical Research Organization / Contract Research OrganizationPHARMAIGNITE100% (1)
- Tablet Coating ProblemsДокумент6 страницTablet Coating ProblemsAnup Bajracharya100% (2)
- Cosmiderma CapsuleДокумент3 страницыCosmiderma Capsulehk_scribdОценок пока нет
- SOP 795 ChecklistДокумент5 страницSOP 795 ChecklistShailendra PatilОценок пока нет
- Formulation and Evaluation of Fast Dissolving Tablet Containing Domperidone Ternary Solid DispersionДокумент9 страницFormulation and Evaluation of Fast Dissolving Tablet Containing Domperidone Ternary Solid DispersionKimia farma AntangОценок пока нет
- 10 3390@pharmaceutics12020151Документ19 страниц10 3390@pharmaceutics12020151Faiqah Fikriyyah AhmadОценок пока нет
- MECFS Clinician Coalition Treatment Recs V1Документ9 страницMECFS Clinician Coalition Treatment Recs V1Emilie ChateletОценок пока нет
- Ranbaxy Laboratories LimitedДокумент9 страницRanbaxy Laboratories LimitedMaroof BaigОценок пока нет