Вам также может понравиться
- Issues in Eye CareДокумент4 страницыIssues in Eye CareMohamed OmerОценок пока нет
- Drugs Affecting Milk Supply During LactationДокумент3 страницыDrugs Affecting Milk Supply During LactationMohamed OmerОценок пока нет
- Pros CarДокумент7 страницPros CarMohamed OmerОценок пока нет
- Physician-Assisted Suicide From A Patient's PerspectiveДокумент1 страницаPhysician-Assisted Suicide From A Patient's PerspectiveMohamed OmerОценок пока нет
- How Do I Copy Ahow Do I Copy A Copy Protected Web Page Copy Protected Web PageДокумент21 страницаHow Do I Copy Ahow Do I Copy A Copy Protected Web Page Copy Protected Web PageMohamed Omer33% (6)
- Comparative Study of the Efficacy and Tolerability of Dihydroartemisinin-piperaquine-trimethoprim Versus Artemether-lumefantrine in the Treatment of Uncomplicated Plasmodium Falciparum Malaria in Cameroon,Документ9 страницComparative Study of the Efficacy and Tolerability of Dihydroartemisinin-piperaquine-trimethoprim Versus Artemether-lumefantrine in the Treatment of Uncomplicated Plasmodium Falciparum Malaria in Cameroon,Mohamed OmerОценок пока нет
- An Update On Antithrombotic Medicines - What Does Primary Care Need To KnowДокумент3 страницыAn Update On Antithrombotic Medicines - What Does Primary Care Need To KnowMohamed OmerОценок пока нет
- All About Gout and TreatmentДокумент2 страницыAll About Gout and TreatmentMohamed OmerОценок пока нет
- Managing Patients With Type 2 Diabetes-From Lifestyle To InsulinДокумент11 страницManaging Patients With Type 2 Diabetes-From Lifestyle To InsulinMohamed OmerОценок пока нет
- A Review of Statin Use and MonitoringДокумент2 страницыA Review of Statin Use and MonitoringMohamed OmerОценок пока нет
- Q&A The Story On The Zika Virus and Microcephaly So FarДокумент3 страницыQ&A The Story On The Zika Virus and Microcephaly So FarMohamed OmerОценок пока нет
- Oncology Endpoints in A Changing Landscape-P&T Magazine SupplementДокумент12 страницOncology Endpoints in A Changing Landscape-P&T Magazine SupplementMohamed OmerОценок пока нет
- Insulin - Pharmacology, Types of Regimens, and AdjustmentsДокумент24 страницыInsulin - Pharmacology, Types of Regimens, and AdjustmentsMohamed OmerОценок пока нет
- Pharmacy & Therapeutics (P&T) Journal-February 2016Документ53 страницыPharmacy & Therapeutics (P&T) Journal-February 2016Mohamed OmerОценок пока нет
- Saudi Arabia's Foreign Policy On Iran and The Proxy WarДокумент10 страницSaudi Arabia's Foreign Policy On Iran and The Proxy WarMohamed OmerОценок пока нет
- HAAD Application How To ApplyДокумент22 страницыHAAD Application How To ApplyMohamed OmerОценок пока нет
- Recomendaciones Practicas para El Uso de AnticonceptivosДокумент64 страницыRecomendaciones Practicas para El Uso de AnticonceptivosLeonardo Antonio Medina AguileraОценок пока нет
- Sudanese Elections Show Significant DeficienciesДокумент11 страницSudanese Elections Show Significant DeficienciesMohamed OmerОценок пока нет
- Ceu Guidance Drug Interactions HormonalДокумент35 страницCeu Guidance Drug Interactions Hormonaljuno ykОценок пока нет
- The Geopolitics of IranДокумент60 страницThe Geopolitics of IranMohamed OmerОценок пока нет
- Progestogen-Only Injectable ContraceptionДокумент40 страницProgestogen-Only Injectable ContraceptionMohamed OmerОценок пока нет
- In Search of Stability Saudi Arabia and The Arab SpringДокумент24 страницыIn Search of Stability Saudi Arabia and The Arab SpringMohamed OmerОценок пока нет
- Adherence To TreatmentДокумент11 страницAdherence To TreatmentMohamed OmerОценок пока нет
- Yemeni Ran SaudiДокумент15 страницYemeni Ran SaudicountofmontecristoОценок пока нет
- Pharmaceutical References and Learning Resources PDFДокумент4 страницыPharmaceutical References and Learning Resources PDFMohamed OmerОценок пока нет
- Torn Yemen Bleeds in Saudi-Iranian Proxy WarДокумент3 страницыTorn Yemen Bleeds in Saudi-Iranian Proxy WarMohamed OmerОценок пока нет
- The Case of The Ethiopian Renaissance - (Nile) DamДокумент18 страницThe Case of The Ethiopian Renaissance - (Nile) DamMohamed OmerОценок пока нет
- Yemen, Saudi Arabia and The Gulf States-Elite PoliticsДокумент20 страницYemen, Saudi Arabia and The Gulf States-Elite PoliticsMohamed OmerОценок пока нет
- Egypt, Ethiopia Headed For War Over WaterДокумент3 страницыEgypt, Ethiopia Headed For War Over WaterMohamed OmerОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- CV Petrangolini enДокумент8 страницCV Petrangolini enTeresa PetrangoliniОценок пока нет
- Interpretation, Taylor & Francis Publiser, London.: Daftar PustakaДокумент3 страницыInterpretation, Taylor & Francis Publiser, London.: Daftar PustakaAnonymous 5K38SwLОценок пока нет
- Perkembangan Bentuk Sedian FarmasiДокумент86 страницPerkembangan Bentuk Sedian FarmasiElviana NoerdianningsihОценок пока нет
- Pharma Companies PuneДокумент3 страницыPharma Companies PuneManoj RamakrishnanОценок пока нет
- EngДокумент5 страницEngRif'atul Alfiyah100% (1)
- Interventions To Improve The Appropriate Use ofДокумент213 страницInterventions To Improve The Appropriate Use ofFarmacia Clínica FES ZaragozaОценок пока нет
- Pharmacy Board ExamsДокумент10 страницPharmacy Board Examsyayooo200467% (6)
- SMF Update Barang 03 Oktober 2022Документ52 страницыSMF Update Barang 03 Oktober 2022Apotek Ibnu RusydОценок пока нет
- TOS - BiopharmaceuticsДокумент6 страницTOS - BiopharmaceuticsApril Mergelle LapuzОценок пока нет
- At The Pharmacy British English TeacherДокумент10 страницAt The Pharmacy British English Teachermr.88nobody88Оценок пока нет
- Rs. 8200 Crore Group Dealing in Pharmaceuticals and Power Based in AhmedabadДокумент33 страницыRs. 8200 Crore Group Dealing in Pharmaceuticals and Power Based in AhmedabadBenor DesaiОценок пока нет
- Faktor-Faktor Yang Mempengaruhi Tuberculosis Multidrug Resistance (TB MDR)Документ9 страницFaktor-Faktor Yang Mempengaruhi Tuberculosis Multidrug Resistance (TB MDR)Dian RohmayantiОценок пока нет
- Clin Pharm ReviewДокумент84 страницыClin Pharm ReviewCristine ChubiboОценок пока нет
- Drug Utilization Review PDFДокумент7 страницDrug Utilization Review PDFDimas CendanaОценок пока нет
- The Development Manual of JamaicaДокумент14 страницThe Development Manual of JamaicaEverton J. O. SmithОценок пока нет
- Life Declaration - 30-03-2017Документ1 страницаLife Declaration - 30-03-2017Ananda Vijayasarathy0% (1)
- CMC Changes and Regulatory ReportingДокумент5 страницCMC Changes and Regulatory Reportingexicial87Оценок пока нет
- Full Product Catalog: Updated: 8/31/2020Документ178 страницFull Product Catalog: Updated: 8/31/2020Sunil Murkikar (GM - PMI Quality Operations)Оценок пока нет
- 08262010Документ31 страница08262010online4049Оценок пока нет
- Group2 DPDD ReportДокумент35 страницGroup2 DPDD ReportPralav RishuОценок пока нет
- CEPP National Audit - Focus On Antibiotic PrescribingДокумент33 страницыCEPP National Audit - Focus On Antibiotic PrescribingmedicembuОценок пока нет
- Anaesthetic Drugs Cheat SheetsДокумент2 страницыAnaesthetic Drugs Cheat SheetsPkern100% (3)
- Farmakologi KlinikДокумент21 страницаFarmakologi KlinikagniajolandaОценок пока нет
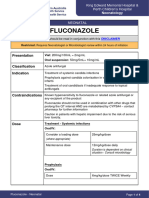
- FluconazoleДокумент4 страницыFluconazoleeucaОценок пока нет
- History and Evolution of PharmacyДокумент96 страницHistory and Evolution of PharmacySamuel Arellano100% (1)
- PV in India Good ArticleДокумент8 страницPV in India Good ArticleAnonymous ceYk4p4Оценок пока нет
- Sma Drug Pipeline: Basic Research Seed IdeasДокумент1 страницаSma Drug Pipeline: Basic Research Seed IdeassvaleravnОценок пока нет
- SoftGel Capsule Part 2Документ109 страницSoftGel Capsule Part 2pharmashri53990% (1)
- Anti-Cancer Drugs: Generic Name Strength SR. NO. Formulation TypeДокумент4 страницыAnti-Cancer Drugs: Generic Name Strength SR. NO. Formulation TypeqaseemОценок пока нет
- Assessment of Glycosylated Hemoglobin Outcomes Following An Enhanced Medication Therapy Management Service Via TelehealthДокумент7 страницAssessment of Glycosylated Hemoglobin Outcomes Following An Enhanced Medication Therapy Management Service Via Telehealthjndelamora18Оценок пока нет