Вам также может понравиться
- Haq Dan Bati1Документ9 страницHaq Dan Bati1Naomi Pradita YuwanaОценок пока нет
- PDF DocumentДокумент44 страницыPDF DocumentBintangemonОценок пока нет
- Acute Bronchitis in Adults - UpToDateДокумент41 страницаAcute Bronchitis in Adults - UpToDateEnrique Vazquez RodriguezОценок пока нет
- Pediatric Community-Acquired Pneumonia: Causes, Symptoms & TreatmentДокумент43 страницыPediatric Community-Acquired Pneumonia: Causes, Symptoms & TreatmentRazel Kinette AzotesОценок пока нет
- Bron Quit IsДокумент19 страницBron Quit IsFranco Fabricio CarpioОценок пока нет
- Acute Bronchitis by UpToDateДокумент10 страницAcute Bronchitis by UpToDateJavieraAlondraDiazОценок пока нет
- Childhood Pneumonia Diagnosis and TreatmentДокумент65 страницChildhood Pneumonia Diagnosis and TreatmentYemata HailuОценок пока нет
- Addis Ababa University: Collage of Health Science Pediatrics and Neonatology On PneumoniaДокумент21 страницаAddis Ababa University: Collage of Health Science Pediatrics and Neonatology On PneumoniaCheru DugaseОценок пока нет
- Case Study PcapДокумент3 страницыCase Study PcapClaire PalaciosОценок пока нет
- The Wheezing Infant: Airway Problems in ChildrenДокумент4 страницыThe Wheezing Infant: Airway Problems in ChildrenDenise DelaneyОценок пока нет
- Referensi 4 BronchiolitisДокумент9 страницReferensi 4 Bronchiolitisaswad 0008Оценок пока нет
- Bronchitis PathophysiologyДокумент23 страницыBronchitis PathophysiologyRama Setya Bagaskara100% (2)
- Respiratory System DisordersДокумент9 страницRespiratory System Disordersasop06Оценок пока нет
- BronchioitisДокумент24 страницыBronchioitismitiku aberaОценок пока нет
- Pediatric Pneumonia: Causes, Presentation and ManagementДокумент10 страницPediatric Pneumonia: Causes, Presentation and Managementko naythweОценок пока нет
- Case Study PNEUMONIAДокумент40 страницCase Study PNEUMONIAHomework PingОценок пока нет
- Chapter 1Документ30 страницChapter 1Ayro Business CenterОценок пока нет
- Pediatric Lower Respiratory InfectionsДокумент27 страницPediatric Lower Respiratory InfectionsAzmachamberAzmacareОценок пока нет
- Acute Respiratory InfectionДокумент28 страницAcute Respiratory InfectionMazharОценок пока нет
- Chapter 4 BronchiectasisДокумент10 страницChapter 4 BronchiectasisAlmira SiamОценок пока нет
- PAEDIATRICS Notes 3 Update PDFДокумент69 страницPAEDIATRICS Notes 3 Update PDFMateen ShukriОценок пока нет
- Wae'l Hayajneh: PneumoniaДокумент14 страницWae'l Hayajneh: PneumoniaRashed ShatnawiОценок пока нет
- 18 UpToDate NeumoníaДокумент113 страниц18 UpToDate NeumoníaAl DavisОценок пока нет
- REQ - PneumoniaДокумент6 страницREQ - PneumoniaAira AgolongОценок пока нет
- Bronchiectasis: DR Budi Enoch SPPDДокумент21 страницаBronchiectasis: DR Budi Enoch SPPDVito CuyОценок пока нет
- Otitis MediaДокумент1 страницаOtitis MediaThan Ramile Dela CruzОценок пока нет
- Growth Chest InfectionsДокумент18 страницGrowth Chest InfectionsjibiannieОценок пока нет
- PneumoniaДокумент68 страницPneumoniaJelmalyn Basali100% (1)
- Clinical Presentation and Diagnosis of Pneumocystis Pulmonary Infection in HIVДокумент42 страницыClinical Presentation and Diagnosis of Pneumocystis Pulmonary Infection in HIVmariano villavicencioОценок пока нет
- CAP in Children: Clinical Features & DiagnosisДокумент51 страницаCAP in Children: Clinical Features & DiagnosisCarolina Morales SuarezОценок пока нет
- Diagnosis Banding I. BronkopneumoniaДокумент20 страницDiagnosis Banding I. BronkopneumoniaHijriah SyafitriОценок пока нет
- lec.2 respirotary system saifДокумент19 страницlec.2 respirotary system saifs2111110520Оценок пока нет
- Acute CoughДокумент7 страницAcute CoughShafira PuspadinaОценок пока нет
- Bronchopneumonia: Causes, Symptoms and TreatmentДокумент2 страницыBronchopneumonia: Causes, Symptoms and TreatmentJanna FavilaОценок пока нет
- Pneumonia Patterns and Causes in Immunocompetent PatientsДокумент12 страницPneumonia Patterns and Causes in Immunocompetent PatientsSeftiana SaftariОценок пока нет
- Sam CD Asthma ReciveredДокумент36 страницSam CD Asthma ReciveredDr. Muha. Hasan Mahbub-Ur-RahmanОценок пока нет
- BronchiolitisДокумент5 страницBronchiolitisreshianeОценок пока нет
- Management of recurrent preschool wheezeДокумент9 страницManagement of recurrent preschool wheezecarlaОценок пока нет
- A. Synthesis of The Disease 1) Definition of The Disease (Book-Based)Документ11 страницA. Synthesis of The Disease 1) Definition of The Disease (Book-Based)glmachic021Оценок пока нет
- Acute Laryngitis and Croup: Diagnosis and TreatmentДокумент5 страницAcute Laryngitis and Croup: Diagnosis and TreatmentIOSR Journal of PharmacyОценок пока нет
- S. Pneumoniae Produces Local Edema That Aids in The Proliferation of Organisms and TheirДокумент7 страницS. Pneumoniae Produces Local Edema That Aids in The Proliferation of Organisms and TheirKadek Soga Prayaditya PutraОценок пока нет
- Chronic Cough in Children: Causes and TreatmentДокумент8 страницChronic Cough in Children: Causes and TreatmentNajla N ShОценок пока нет
- Understanding Bronchiectasis: Causes, Diagnosis and TreatmentДокумент7 страницUnderstanding Bronchiectasis: Causes, Diagnosis and TreatmentrecursitaОценок пока нет
- Group A May Intake WorkДокумент14 страницGroup A May Intake WorkdeblackaОценок пока нет
- Chapter VI.11. Pulmonary Infections: Case Based Pediatrics For Medical Students and ResidentsДокумент8 страницChapter VI.11. Pulmonary Infections: Case Based Pediatrics For Medical Students and ResidentsصثقيفبلغاعОценок пока нет
- Pneumonia Is An: ClinicalДокумент13 страницPneumonia Is An: ClinicaldfgsfsfssdОценок пока нет
- 3 - PneumoniaДокумент6 страниц3 - PneumoniaAmmar AlnajjarОценок пока нет
- Pneumonia 1Документ17 страницPneumonia 1Jonathan katanaОценок пока нет
- Lec 9 Respiratory Disorders Part 2Документ11 страницLec 9 Respiratory Disorders Part 2iam2117Оценок пока нет
- Community-Acquired Pneumonia in Children: Clinical Features and Diagnosis - UpToDateДокумент62 страницыCommunity-Acquired Pneumonia in Children: Clinical Features and Diagnosis - UpToDateYeidhy Karin Cayo CoñezОценок пока нет
- Bacteria Infection of The Respiratory TractДокумент8 страницBacteria Infection of The Respiratory TractChidi EmmanuelОценок пока нет
- Pertussis. Unfortunately, in About Half The Cases, The Specific Cause of Bronchiectasis RemainsДокумент14 страницPertussis. Unfortunately, in About Half The Cases, The Specific Cause of Bronchiectasis RemainsAnonymous qwH3D0KrpОценок пока нет
- 3 PneumoniaДокумент17 страниц3 PneumoniaMohamed Na3eemОценок пока нет
- Bronchitis Vs BronchiolitisДокумент52 страницыBronchitis Vs BronchiolitisUngku Hajar Nur AthirahОценок пока нет
- Pneumonia Is AnДокумент9 страницPneumonia Is Ansandro2000Оценок пока нет
- Medical Mnemonic Sketches : Pulmonary DiseasesОт EverandMedical Mnemonic Sketches : Pulmonary DiseasesОценок пока нет
- Diagnosis and Treatment of Chronic CoughОт EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoОценок пока нет
- Lung Infections, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandLung Infections, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Bronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandBronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Fever Headache Dizziness Seizure Nausea Vomiting: - X Cough DOB Constipation Diarrhea - X Abd. Pain: Location: QualityДокумент2 страницыFever Headache Dizziness Seizure Nausea Vomiting: - X Cough DOB Constipation Diarrhea - X Abd. Pain: Location: QualityJohnVincentPagadduОценок пока нет
- Critical Appraisal by John Vincent Pagaddu, M.D.Документ91 страницаCritical Appraisal by John Vincent Pagaddu, M.D.JohnVincentPagadduОценок пока нет
- Local Mechanisms Affect MAPДокумент1 страницаLocal Mechanisms Affect MAPJohnVincentPagadduОценок пока нет
- Self-Reliance and ProcurementДокумент16 страницSelf-Reliance and ProcurementJohnVincentPagadduОценок пока нет
- Mollusc I Pox VirusДокумент2 страницыMollusc I Pox VirusJohnVincentPagadduОценок пока нет
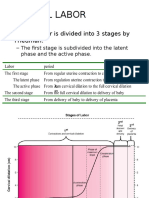
- Normal Labor: - Normal Labor Is Divided Into 3 Stages by FriedmanДокумент13 страницNormal Labor: - Normal Labor Is Divided Into 3 Stages by FriedmanJohnVincentPagadduОценок пока нет
- Systemic Response To InjuryДокумент15 страницSystemic Response To InjuryJohnVincentPagaddu100% (1)
- ENC Part IДокумент6 страницENC Part IJohnVincentPagadduОценок пока нет
- The BronchiДокумент64 страницыThe BronchiJohnVincentPagadduОценок пока нет
- Bio StatisticsДокумент16 страницBio StatisticsJohnVincentPagadduОценок пока нет
- HealthДокумент5 страницHealthJohnVincentPagadduОценок пока нет
- Sanctity and ScarcityДокумент33 страницыSanctity and ScarcityJohnVincentPagaddu100% (1)
- Types of Mixtures LabДокумент2 страницыTypes of Mixtures LabJohnVincentPagadduОценок пока нет
- Surgery Ortho TraumaДокумент8 страницSurgery Ortho TraumaJohnVincentPagadduОценок пока нет
- Derma Sample Exam For Practicals (Skin and Lesions)Документ42 страницыDerma Sample Exam For Practicals (Skin and Lesions)JohnVincentPagaddu100% (1)
- Population Mortality: Reported By: Group Four TFEG1 Biology 160 Lab AY 2010-2011 2 SemesterДокумент57 страницPopulation Mortality: Reported By: Group Four TFEG1 Biology 160 Lab AY 2010-2011 2 SemesterJohnVincentPagadduОценок пока нет
- Pediaortho Hand OutДокумент119 страницPediaortho Hand OutJohnVincentPagadduОценок пока нет
- Tuberculosis (TB) Blood Test (IGRA) : Minnesota Department of HealthДокумент1 страницаTuberculosis (TB) Blood Test (IGRA) : Minnesota Department of HealthYeon Ae NaritaОценок пока нет
- MUST To KNOW in Clinical ChemistryДокумент1 страницаMUST To KNOW in Clinical ChemistryEdel BinasoyОценок пока нет
- (Methods in Microbiology 17) P.M. Bennett and J. Grinsted (Eds.) - Plasmid Technology-Academic Press (1984) PDFДокумент320 страниц(Methods in Microbiology 17) P.M. Bennett and J. Grinsted (Eds.) - Plasmid Technology-Academic Press (1984) PDFStella RodicaОценок пока нет
- Rambabu NarvaneniДокумент4 страницыRambabu NarvaneniS291991Оценок пока нет
- Polyomavirus LectureДокумент60 страницPolyomavirus Lecturerggefrm75% (4)
- Microbiology Principles and Explorations 10th Edition Black Test BankДокумент36 страницMicrobiology Principles and Explorations 10th Edition Black Test Bankdavidnelsonseyjdmpoaz100% (12)
- Food Science Catalog FINAL Low ResДокумент29 страницFood Science Catalog FINAL Low ResJohn Deck TanОценок пока нет
- Journal Reading ParuДокумент53 страницыJournal Reading ParuDaniel IvanОценок пока нет
- Which Is Better JJ, Moderna, or PfizerДокумент1 страницаWhich Is Better JJ, Moderna, or PfizerCarl Melvin PobleteОценок пока нет
- Effects of Viral ReplicationДокумент3 страницыEffects of Viral ReplicationSamuel OgaroОценок пока нет
- Covid-19 RTPCR (Sars Cov-2) Throat/Nasal Swab-Haryana : Laboratory Investigation ReportДокумент1 страницаCovid-19 RTPCR (Sars Cov-2) Throat/Nasal Swab-Haryana : Laboratory Investigation ReportkanavОценок пока нет
- Judicial Watch v. National Institutes of Health - Wuhan Case No. 21-cv-00696Документ303 страницыJudicial Watch v. National Institutes of Health - Wuhan Case No. 21-cv-00696John DoeОценок пока нет
- General Characteristics of Bacteria and MollicutesДокумент13 страницGeneral Characteristics of Bacteria and MollicutesPrincess Mehra0% (1)
- Jurnal Nuzul Yustian 14710112Документ8 страницJurnal Nuzul Yustian 14710112nuzul akira tendoОценок пока нет
- Probiotics and Prebiotics: International Journal of Current Research December 2018Документ13 страницProbiotics and Prebiotics: International Journal of Current Research December 2018Maï SsaОценок пока нет
- Municipal Wastewater Treatment ProcessesДокумент34 страницыMunicipal Wastewater Treatment ProcessesHaswanth KolluОценок пока нет
- 2chain of DiseaseДокумент43 страницы2chain of Diseaseyuuki konno100% (1)
- Isolation PrecautionsДокумент13 страницIsolation Precautionsmalyn1218Оценок пока нет
- ImpetigoДокумент16 страницImpetigokikimasyhurОценок пока нет
- EngДокумент244 страницыEngIntan IntanОценок пока нет
- LKPD II-Covid 19 Report TextДокумент2 страницыLKPD II-Covid 19 Report TextNurul Rahmawati100% (2)
- Antibiotic Resistance Essay - Third DraftДокумент5 страницAntibiotic Resistance Essay - Third DraftKevin JohnsenОценок пока нет
- Top 10 Benefits of Environmental Education: 1. Imagination and Enthusiasm Are HeightenedДокумент5 страницTop 10 Benefits of Environmental Education: 1. Imagination and Enthusiasm Are Heightenedsagar mittalОценок пока нет
- Eretemia (Parvovirus 2016)Документ5 страницEretemia (Parvovirus 2016)Yoga MadaniОценок пока нет
- Common ColdДокумент3 страницыCommon ColdshaliniОценок пока нет
- B Cepacia What Is It and Why Is It A ConcernДокумент5 страницB Cepacia What Is It and Why Is It A ConcernBlueSagaОценок пока нет
- Microsoft Office PowerPoint Presentation NouДокумент8 страницMicrosoft Office PowerPoint Presentation NouStavarache LarisaОценок пока нет
- ASTM D4783 - 01 (2021) Standard Test Methods For Resistance of Adhesive Preparations in Container To AttackДокумент4 страницыASTM D4783 - 01 (2021) Standard Test Methods For Resistance of Adhesive Preparations in Container To AttackAbdullah0% (1)
- Parasitology 1Документ18 страницParasitology 1christine delgado100% (2)
- Contaminación de Los Suelos Con Huevos de Toxocara Canis en ParquesДокумент12 страницContaminación de Los Suelos Con Huevos de Toxocara Canis en ParquesJahir QHОценок пока нет