Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Online Magazine On PharmaДокумент19 страницOnline Magazine On Pharmaanish_10677953Оценок пока нет
- Report of MalariaДокумент3 страницыReport of Malariaanish_10677953Оценок пока нет
- Indian Council of Medical ResearchДокумент9 страницIndian Council of Medical Researchkuldeepgju17Оценок пока нет
- Updated List 2014 of DrugsДокумент4 страницыUpdated List 2014 of Drugsanish_10677953Оценок пока нет
- Sanskrit University Sampurnanand Sanskrit University Is An Asian Institution of Higher Learning Located inДокумент2 страницыSanskrit University Sampurnanand Sanskrit University Is An Asian Institution of Higher Learning Located inanish_10677953Оценок пока нет
- Pdfs CritspinManualДокумент17 страницPdfs CritspinManualanish_10677953Оценок пока нет
- 11431451965Документ1 страница11431451965PrashantVedwanОценок пока нет
- Untitled DocumentДокумент2 страницыUntitled Documentanish_10677953Оценок пока нет
- Supply List of Mesa LabДокумент2 страницыSupply List of Mesa Labanish_10677953Оценок пока нет
- 2014 04 22 02 39 47 How-to-apply-OfflineДокумент1 страница2014 04 22 02 39 47 How-to-apply-Offlineanish_10677953Оценок пока нет
- University Grants CommisionДокумент1 страницаUniversity Grants Commisionanish_10677953Оценок пока нет
- Diagnostics Report Form 20130115Документ5 страницDiagnostics Report Form 20130115anish_10677953Оценок пока нет
- Darjeeling Travel GuideДокумент16 страницDarjeeling Travel Guideanish_10677953Оценок пока нет
- Roll Number 653298: Ukssv %& VH FKHZ Izr SD Iz'U I GSRQ Vyx&Vyx Izos'K I E Miflfkfr I Mkmuyksm DjsaaДокумент1 страницаRoll Number 653298: Ukssv %& VH FKHZ Izr SD Iz'U I GSRQ Vyx&Vyx Izos'K I E Miflfkfr I Mkmuyksm Djsaaanish_10677953Оценок пока нет
- Project On Body LanguageДокумент51 страницаProject On Body Languagevikash88% (8)
- Guru Ghasidas Vishwavidyalaya Bilaspur (C.G.)Документ4 страницыGuru Ghasidas Vishwavidyalaya Bilaspur (C.G.)anish_10677953Оценок пока нет
- Application Form For Non-Teaching Contractual Engagement1Документ2 страницыApplication Form For Non-Teaching Contractual Engagement1AnamikaShuklaОценок пока нет
- BSNL Bill 1Документ1 страницаBSNL Bill 1anish_10677953Оценок пока нет
- Marketing Brand Role in Buying Behaviour of YouthДокумент61 страницаMarketing Brand Role in Buying Behaviour of Youthanish_10677953Оценок пока нет
- 20.5.14-Bachelor of Education (Special Education - Hearing Impaired)Документ14 страниц20.5.14-Bachelor of Education (Special Education - Hearing Impaired)anish_10677953Оценок пока нет
- Schedule yДокумент58 страницSchedule yanish_10677953Оценок пока нет
- Net JRFДокумент10 страницNet JRFB. Rajeev Kungur100% (2)
- Aryans Institute of Management & TechnologyДокумент53 страницыAryans Institute of Management & TechnologyvikashОценок пока нет
- NABARDДокумент110 страницNABARDKini Shi100% (1)
- BD Product ListДокумент48 страницBD Product Listanish_10677953100% (1)
- Employee WelfareДокумент76 страницEmployee Welfareanish_10677953Оценок пока нет
- The Concept of ValueДокумент17 страницThe Concept of Valueanish_10677953Оценок пока нет
- STRESS MnagmentДокумент107 страницSTRESS Mnagmentanish_10677953Оценок пока нет
- No Content Page No 1 1 1.1: Employee Performanc Objectives of Performance AppraisalДокумент2 страницыNo Content Page No 1 1 1.1: Employee Performanc Objectives of Performance Appraisalanish_10677953Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Conatct ListДокумент58 страницConatct ListBadal Bhattacharya50% (2)
- RanbaxyДокумент18 страницRanbaxyDipankar PandeyОценок пока нет
- Case 6.3 "Off-Label" Marketing: GROUP 8 - Lecture: Alang ThoДокумент12 страницCase 6.3 "Off-Label" Marketing: GROUP 8 - Lecture: Alang ThoNganОценок пока нет
- Guideline For Drug Master FilesДокумент33 страницыGuideline For Drug Master FilesRambabu komati - QA100% (3)
- Homework1 SirrolaДокумент4 страницыHomework1 Sirrolarniyatee90Оценок пока нет
- Conference Delegate Wish ListДокумент55 страницConference Delegate Wish ListThinkLink, Foreign Affairs www.thinklk.comОценок пока нет
- PHARMA COMPANIES Details With Websites 09Документ1 страницаPHARMA COMPANIES Details With Websites 09Irfan SheikОценок пока нет
- ShimadzuДокумент17 страницShimadzuMuhammed FarrukhОценок пока нет
- Franklin Fink CVДокумент27 страницFranklin Fink CVThe Florida Times-UnionОценок пока нет
- Economics of The Pharmaceutical IndustryДокумент12 страницEconomics of The Pharmaceutical IndustrySambasiva RaoОценок пока нет
- Pharmaceutical EngineeringДокумент5 страницPharmaceutical EngineeringmikebluberryОценок пока нет
- The Regulatory Trends: Cross-Contamination in Drug ManufacturingДокумент9 страницThe Regulatory Trends: Cross-Contamination in Drug Manufacturinglina kharratОценок пока нет
- General Profile of Pharmaceutical CompaniesДокумент3 страницыGeneral Profile of Pharmaceutical CompaniesHaile Kassa100% (1)
- Regen PDFДокумент6 страницRegen PDFaditisinghaniaОценок пока нет
- Trends in Oncology Business DevelopmentДокумент25 страницTrends in Oncology Business DevelopmentSheltie ForeverОценок пока нет
- ATH Stocks, Technical Analysis ScannerДокумент4 страницыATH Stocks, Technical Analysis Scanneromkarambale1Оценок пока нет
- The Road To Digital Success in Pharma - McKinsey & CompanyДокумент10 страницThe Road To Digital Success in Pharma - McKinsey & CompanyharshalОценок пока нет
- PDFДокумент156 страницPDFvidhi hiteshОценок пока нет
- PM Journal1Документ10 страницPM Journal1gireesh_babuОценок пока нет
- Data Transaksi Obat Sanbe SD 06032019Документ2 031 страницаData Transaksi Obat Sanbe SD 06032019desiduwiОценок пока нет
- Trump Legal CBD OilДокумент9 страницTrump Legal CBD OilChiefJustice Middleton100% (1)
- Mukund SДокумент19 страницMukund SHajime HikariОценок пока нет
- Bonus Product Sales April-2023Документ3 страницыBonus Product Sales April-2023Mahbub Alam SarkerОценок пока нет
- Vol 19.2 Dementia.2013Документ208 страницVol 19.2 Dementia.2013Martoiu MariaОценок пока нет
- The Searle Company (SEARL) - Reinstating With A BuyДокумент17 страницThe Searle Company (SEARL) - Reinstating With A BuySHAHZAIB -Оценок пока нет
- Senario Case StudyДокумент19 страницSenario Case Studymaya100% (1)
- Drug Policy 2017 (Medex - Com.bd)Документ64 страницыDrug Policy 2017 (Medex - Com.bd)মোঃ এমদাদুল হকОценок пока нет
- Daftar Peoduk SanbeДокумент7 страницDaftar Peoduk SanbeDuduSaepudinОценок пока нет
- Revision 1 2021Документ23 страницыRevision 1 2021Rin AkaneОценок пока нет
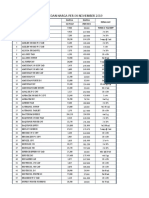
- Imcops Price List From 01 - 11 - 2015 PDFДокумент26 страницImcops Price List From 01 - 11 - 2015 PDFGoutham PillaiОценок пока нет