Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Dr. A. Ria KurniawatiДокумент1 страницаDr. A. Ria KurniawatiDesintha RachmanОценок пока нет
- 1Документ1 страница1Desintha RachmanОценок пока нет
- Pengunduran Diri AnggaДокумент1 страницаPengunduran Diri AnggaDesintha RachmanОценок пока нет
- Rekapitulasi Akses AnggotaДокумент1 страницаRekapitulasi Akses AnggotaDesintha RachmanОценок пока нет
- Dok Baru 2019-02-05 16.57.09 PDFДокумент1 страницаDok Baru 2019-02-05 16.57.09 PDFDesintha RachmanОценок пока нет
- Dok Baru 2019-02-05 16.57.09Документ1 страницаDok Baru 2019-02-05 16.57.09Desintha RachmanОценок пока нет
- 2592 5623 1 SMДокумент11 страниц2592 5623 1 SMMuthia FauzanОценок пока нет
- JNJ IlolДокумент1 страницаJNJ IlolDesintha RachmanОценок пока нет
- Vrfegr 5 TW 5 T 54Документ1 страницаVrfegr 5 TW 5 T 54Desintha RachmanОценок пока нет
- JNJ IlolДокумент1 страницаJNJ IlolDesintha RachmanОценок пока нет
- 8.4.3.EP.1.SK Tentang Sistem PengkodeanДокумент9 страниц8.4.3.EP.1.SK Tentang Sistem PengkodeanDesintha RachmanОценок пока нет
- Vrfegr 5 TW 5 T 54Документ1 страницаVrfegr 5 TW 5 T 54Desintha RachmanОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Announcement List Displayed Poster 32nd ASMIHAДокумент36 страницAnnouncement List Displayed Poster 32nd ASMIHADewi AmeliaОценок пока нет
- Aherrera NotesДокумент213 страницAherrera NotesVerna Santiago71% (7)
- Cardiac Monitoring Pocket CardДокумент2 страницыCardiac Monitoring Pocket Cardpurplefeather_14100% (1)
- Latin 2Документ29 страницLatin 2ShreyaОценок пока нет
- Does Obesity Cause Type 2 Diabetes MellitusДокумент5 страницDoes Obesity Cause Type 2 Diabetes Mellitusthebrotherhood2014Оценок пока нет
- Finals Reviewer 102517Документ20 страницFinals Reviewer 102517Kyla R. PinedaОценок пока нет
- Miocarditis Por Clozapina Ronaldson2017 Revisión SistematicaДокумент19 страницMiocarditis Por Clozapina Ronaldson2017 Revisión SistematicaAlejandro PiscitelliОценок пока нет
- Tenecteplase Thrombolysis For Acute IschemicДокумент12 страницTenecteplase Thrombolysis For Acute IschemicRicardo AcostaОценок пока нет
- Case Clerking MIДокумент13 страницCase Clerking MIKhairi Abd RahimОценок пока нет
- 1013 Vasoactive Agents in ShockДокумент20 страниц1013 Vasoactive Agents in Shockrogelio cruzОценок пока нет
- Case Study On ARFДокумент33 страницыCase Study On ARFKaku ManishaОценок пока нет
- INC Vs RosalesДокумент2 страницыINC Vs RosalesMiw CortesОценок пока нет
- Anatomia FacialДокумент10 страницAnatomia FacialIgor NatanyoОценок пока нет
- Test Bank For Phlebotomy Handbook 9th Edition Diana Garza Kathleen Becan McbrideДокумент14 страницTest Bank For Phlebotomy Handbook 9th Edition Diana Garza Kathleen Becan Mcbrideanthonyelliscnjswramob100% (24)
- Tetralogy of Fallot NCPДокумент6 страницTetralogy of Fallot NCPHarlene Joyce ReyОценок пока нет
- Gastrointestinal System Disorders: Anna Marie M. Ventulan, MD, DPPS, DPSNBMДокумент85 страницGastrointestinal System Disorders: Anna Marie M. Ventulan, MD, DPPS, DPSNBMLyn LynОценок пока нет
- Zomen in CKDДокумент12 страницZomen in CKDClaudiu BalabanОценок пока нет
- Cumin (Cuminum Cyminum) and Black CuminДокумент16 страницCumin (Cuminum Cyminum) and Black Cuminharoon arshadОценок пока нет
- 800 +MCQs-ONLY SUCCESS MRCS-A (UPDATED)Документ378 страниц800 +MCQs-ONLY SUCCESS MRCS-A (UPDATED)DrTawfik Shabaka100% (1)
- Pregnancy Induced Hypertension (PIH) : Case Scenario 4Документ4 страницыPregnancy Induced Hypertension (PIH) : Case Scenario 4Mae Arra Lecobu-anОценок пока нет
- The Mammalian Heart PP WorksheetДокумент2 страницыThe Mammalian Heart PP WorksheetnremeckiОценок пока нет
- SAS #16 NUR 151: Your Email Will Be Recorded When You Submit This FormДокумент7 страницSAS #16 NUR 151: Your Email Will Be Recorded When You Submit This FormA.Оценок пока нет
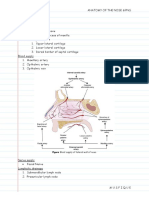
- Anatomy of The Nose & Paranasal Air SinusesДокумент4 страницыAnatomy of The Nose & Paranasal Air SinusesMusfique RashidОценок пока нет
- SympatheticДокумент10 страницSympatheticSharneeshriyaОценок пока нет
- Hypertension Nursing Care PlanДокумент2 страницыHypertension Nursing Care PlanCj LowryОценок пока нет
- 2015 Anesthesia For Genetic, Metabolic, & Dysmorphic Syndromes of Childhood PDFДокумент965 страниц2015 Anesthesia For Genetic, Metabolic, & Dysmorphic Syndromes of Childhood PDFHidayati IdaОценок пока нет
- Case 3Документ7 страницCase 3Edilyn BalicaoОценок пока нет
- Step 1 ShartzДокумент333 страницыStep 1 ShartzDaniella Vazquez100% (1)
- A Case Study On Uterine FibroidsДокумент24 страницыA Case Study On Uterine FibroidsAj Go100% (1)
- Hypersensitivity To Nickel in A Patient Treated With Coil Embolization For Pelvic Congestion SyndromeДокумент3 страницыHypersensitivity To Nickel in A Patient Treated With Coil Embolization For Pelvic Congestion SyndromeJack GuccioneОценок пока нет