Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Alice Hoffman - Green AngelДокумент24 страницыAlice Hoffman - Green AngelHristiyana Yotova71% (14)
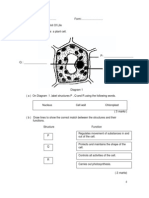
- Name : .. Chapter 2 - Cell As A Unit ofДокумент17 страницName : .. Chapter 2 - Cell As A Unit ofRozaini Othman81% (27)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- DR 890 Colorimeter Procedures ManualДокумент614 страницDR 890 Colorimeter Procedures ManualArmin MajerОценок пока нет
- Opening RitualДокумент17 страницOpening RitualTracy CrockettОценок пока нет
- Flowera, Fruits and SeedsДокумент66 страницFlowera, Fruits and SeedsNikkaMontil100% (1)
- EDMU 520 Phonics Lesson ObservationДокумент6 страницEDMU 520 Phonics Lesson ObservationElisa FloresОценок пока нет
- PAPER 3 (Set1) QuestionДокумент9 страницPAPER 3 (Set1) Questionjess2025Оценок пока нет
- Parasympathetic Nervous SystemДокумент5 страницParasympathetic Nervous SystemRay Peramathevan RavendranОценок пока нет
- Chemistry Basics (Atoms, Electrons, Periodic Table, Etc.)Документ2 страницыChemistry Basics (Atoms, Electrons, Periodic Table, Etc.)Ray Peramathevan RavendranОценок пока нет
- CH 14 Inheritance TeacherДокумент20 страницCH 14 Inheritance TeacherRay Peramathevan Ravendran100% (3)
- Tips Final CDLДокумент17 страницTips Final CDLRay Peramathevan RavendranОценок пока нет
- Diagram shows three organism skeleton typesДокумент10 страницDiagram shows three organism skeleton typesRay Peramathevan RavendranОценок пока нет
- Upsr Mock ObjecДокумент4 страницыUpsr Mock ObjecRay Peramathevan RavendranОценок пока нет
- Trial MRSM Biologi SPM 2014 K2 No SkemaДокумент36 страницTrial MRSM Biologi SPM 2014 K2 No SkemaCikgu Faizal80% (5)
- SPM Form 5 Biology Quick Revision KitДокумент7 страницSPM Form 5 Biology Quick Revision KitRay Peramathevan RavendranОценок пока нет
- Safety of blood products threatened by unscreened viruses and bacteriaДокумент1 страницаSafety of blood products threatened by unscreened viruses and bacteriaRay Peramathevan RavendranОценок пока нет
- Parasympathetic Nervous SystemДокумент5 страницParasympathetic Nervous SystemRay Peramathevan RavendranОценок пока нет
- RULE BREAKING BEHAVIOUR QUESTIONNAIREДокумент4 страницыRULE BREAKING BEHAVIOUR QUESTIONNAIREElliyana Natasha YunosОценок пока нет
- Cross-sectional study measures blood lead in Chennai childrenДокумент1 страницаCross-sectional study measures blood lead in Chennai childrenRay Peramathevan RavendranОценок пока нет
- Upsr Mock ObjecДокумент4 страницыUpsr Mock ObjecRay Peramathevan RavendranОценок пока нет
- Chapter 3 Coordination and RespionsesДокумент2 страницыChapter 3 Coordination and RespionsesRay Peramathevan RavendranОценок пока нет
- PREGLED LITERATURE - Primjer Eseja Istraživanja Iz PsihologijeДокумент10 страницPREGLED LITERATURE - Primjer Eseja Istraživanja Iz PsihologijeInes BresicОценок пока нет
- Homeostasis Internal EnvironmentДокумент3 страницыHomeostasis Internal EnvironmentRay Peramathevan RavendranОценок пока нет
- Adolescent Knowledge About Sexually Transmitted.2Документ8 страницAdolescent Knowledge About Sexually Transmitted.2Ray Peramathevan RavendranОценок пока нет
- Plugin-Research Assistant CV Template-1Документ2 страницыPlugin-Research Assistant CV Template-1Arslan MukhtarОценок пока нет
- Mechanism of Action of Guanethidine ExploredДокумент11 страницMechanism of Action of Guanethidine ExploredRay Peramathevan RavendranОценок пока нет
- 79 e 415072 D 1 C 78 D 6 FFДокумент12 страниц79 e 415072 D 1 C 78 D 6 FFRay Peramathevan RavendranОценок пока нет
- tp115 c6Документ24 страницыtp115 c6Ray Peramathevan RavendranОценок пока нет
- By Authority of Legally Binding Document: The United States of AmericaДокумент14 страницBy Authority of Legally Binding Document: The United States of AmericaRay Peramathevan RavendranОценок пока нет
- L2129Документ84 страницыL2129Sohail HanifОценок пока нет
- Form 1 Integrated Science Time: 1H 30minДокумент10 страницForm 1 Integrated Science Time: 1H 30minNg Lay HoonОценок пока нет
- Biologi F4 Final SBP 2007 P2Документ36 страницBiologi F4 Final SBP 2007 P2Ummu SyifakОценок пока нет
- 2009 Up 1 F 1Документ14 страниц2009 Up 1 F 1Cikgu AzamОценок пока нет
- Attitudes Toward Homosexuality Among Peninsula Malaysia University StudentsДокумент62 страницыAttitudes Toward Homosexuality Among Peninsula Malaysia University StudentsRay Peramathevan RavendranОценок пока нет
- Webquest Biotechnology RubricДокумент2 страницыWebquest Biotechnology Rubricapi-556285637Оценок пока нет
- SDSDДокумент114 страницSDSDbhatiasabОценок пока нет
- Clinical Study of Incidence of Extraocular Foreign Bodies in Teritiary HospitalДокумент5 страницClinical Study of Incidence of Extraocular Foreign Bodies in Teritiary HospitalIJAR JOURNALОценок пока нет
- Definite IntegralsДокумент51 страницаDefinite IntegralsKovid BalliОценок пока нет
- Daily Aspirin Therapy Understand The Benefits and RisksДокумент5 страницDaily Aspirin Therapy Understand The Benefits and RisksNicholas OwensОценок пока нет
- VajroliДокумент3 страницыVajroliJithu BayiОценок пока нет
- Christoffel Symbols: PHYS 471: Introduction To Relativity and CosmologyДокумент9 страницChristoffel Symbols: PHYS 471: Introduction To Relativity and Cosmologyarileo3100% (1)
- Chapter 8 SQL Complex QueriesДокумент51 страницаChapter 8 SQL Complex QueriesJiawei TanОценок пока нет
- Almeda v. CaДокумент10 страницAlmeda v. CaRuss TuazonОценок пока нет
- Meena ResumeДокумент3 страницыMeena ResumeAnonymous oEzGNEОценок пока нет
- KNAW Proceedings from 1919-1920Документ481 страницаKNAW Proceedings from 1919-1920Eduardo Salgado EnríquezОценок пока нет
- Learning Competencies For English - Grades 11-12Документ5 страницLearning Competencies For English - Grades 11-12Neo Artajo100% (1)
- A Summer's Reading - Sample Questions With AnswersДокумент11 страницA Summer's Reading - Sample Questions With AnswersRoy SchwartzОценок пока нет
- Seduction As A Manipulation TacticДокумент6 страницSeduction As A Manipulation TacticByrlyne Van DykeDowersОценок пока нет
- Reflection Paper - InternshipДокумент7 страницReflection Paper - Internshipapi-549362324Оценок пока нет
- Coordinates: Primary Practice QuestionsДокумент10 страницCoordinates: Primary Practice QuestionsJames KeruОценок пока нет
- A.T Jones-Great Empires of Prophecy From Babylon To The Fall of RomeДокумент640 страницA.T Jones-Great Empires of Prophecy From Babylon To The Fall of RomeDANTZIE100% (2)
- Compulsive Buying Tendency As A Predictor of Attitudes and PerceptionsДокумент4 страницыCompulsive Buying Tendency As A Predictor of Attitudes and PerceptionsvsharanyaОценок пока нет
- FluteДокумент3 страницыFlutepatrickduka123100% (1)
- Vodafone - Market Research ProposalДокумент4 страницыVodafone - Market Research ProposalNikita Sanghvi100% (2)
- Matrix Software User ManuelДокумент45 страницMatrix Software User ManuelHema SantoshОценок пока нет
- Tanada, Et Al. Vs Angara, Et Al., 272 SCRA 18, GR 118295 (May 2, 1997)Документ3 страницыTanada, Et Al. Vs Angara, Et Al., 272 SCRA 18, GR 118295 (May 2, 1997)Lu CasОценок пока нет
- Nikita S ResumeДокумент2 страницыNikita S ResumeNikita SrivastavaОценок пока нет
- CHAP 1: STATS & SCIENTIFIC METHODДокумент9 страницCHAP 1: STATS & SCIENTIFIC METHODJesheryll ReasОценок пока нет
- Rock and Roll and The American Dream: Essential QuestionДокумент7 страницRock and Roll and The American Dream: Essential QuestionChad HorsleyОценок пока нет