Вам также может понравиться
- 02 Review On Artemisinine Derivatives For Malaria Control TANG Lin-HuaДокумент38 страниц02 Review On Artemisinine Derivatives For Malaria Control TANG Lin-HuaFitri Amelia RizkiОценок пока нет
- Management of Diabetic Foot Ulcers: A ReviewДокумент8 страницManagement of Diabetic Foot Ulcers: A ReviewFitri Amelia RizkiОценок пока нет
- Fundamentals of Oxygen Therapy.6Документ3 страницыFundamentals of Oxygen Therapy.6Fitri Amelia RizkiОценок пока нет
- 2015 Gout Classification CriteriaДокумент12 страниц2015 Gout Classification CriteriaVico RizkytaОценок пока нет
- Clinical and Experimental Advances in Congenital and Paediatric CataractsДокумент16 страницClinical and Experimental Advances in Congenital and Paediatric CataractsFitri Amelia RizkiОценок пока нет
- Antipsychotic Deprescribing Algorithm PDFДокумент2 страницыAntipsychotic Deprescribing Algorithm PDFFitri Amelia RizkiОценок пока нет
- ST T Classification Who ChapterДокумент11 страницST T Classification Who ChapterFitri Amelia RizkiОценок пока нет
- A Trevor's Disease HindawiДокумент9 страницA Trevor's Disease HindawiFitri Amelia RizkiОценок пока нет
- Ecr2015 c-1165Документ28 страницEcr2015 c-1165Fitri Amelia RizkiОценок пока нет
- Infantile CataractДокумент6 страницInfantile Cataractkartini ciatawiОценок пока нет
- RefratДокумент31 страницаRefratFitri Amelia RizkiОценок пока нет
- Ophthalmology Referral GuidelinesДокумент9 страницOphthalmology Referral GuidelinesFitri Amelia RizkiОценок пока нет
- Red Reflex Test: ProcedureДокумент6 страницRed Reflex Test: ProcedureFitri Amelia RizkiОценок пока нет
- Cataract: Care of The Adult Patient WithДокумент43 страницыCataract: Care of The Adult Patient WithAnna Francesca AbarquezОценок пока нет
- Hyphema 2Документ7 страницHyphema 2heidyОценок пока нет
- Amniosentesis Dan CvsДокумент13 страницAmniosentesis Dan CvsFitri Amelia RizkiОценок пока нет
- Glaucoma GuidelinesДокумент28 страницGlaucoma GuidelinesRina RostianaОценок пока нет
- ABJS Volume 4 Issue 1 Pages 2-9Документ8 страницABJS Volume 4 Issue 1 Pages 2-9Fitri Amelia RizkiОценок пока нет
- Cios 4 107 PDFДокумент10 страницCios 4 107 PDFFitri Amelia RizkiОценок пока нет
- Jurnal Konservatif ManagementДокумент5 страницJurnal Konservatif ManagementFitri Amelia RizkiОценок пока нет
- EAU Extended Guidelines 2016 EdnДокумент1 159 страницEAU Extended Guidelines 2016 Ednsamirmohd100% (1)
- THE Pathology OF Osteoclastoma OR Giant-Cell Tumour OF Bone: Willis, London, EnglandДокумент5 страницTHE Pathology OF Osteoclastoma OR Giant-Cell Tumour OF Bone: Willis, London, EnglandFitri Amelia RizkiОценок пока нет
- JurnalДокумент4 страницыJurnalFitri Amelia RizkiОценок пока нет
- The Nervous System: Quicktime™ An D A Tiff (Uncompressed) Decompressor Are Need Ed To See This P IctureДокумент26 страницThe Nervous System: Quicktime™ An D A Tiff (Uncompressed) Decompressor Are Need Ed To See This P IcturecamixxxОценок пока нет
- Emergency Medical Tech PPT Templates StandardДокумент9 страницEmergency Medical Tech PPT Templates StandardFitri Amelia RizkiОценок пока нет
- Virtual Autopsy in Forensic Medicine-00085892Документ4 страницыVirtual Autopsy in Forensic Medicine-00085892Fitri Amelia RizkiОценок пока нет
- Jurnal 2 - TBДокумент8 страницJurnal 2 - TBFitri Amelia RizkiОценок пока нет
- Research Article: Outcome Predictors in First-Ever Ischemic Stroke Patients: A Population-Based StudyДокумент9 страницResearch Article: Outcome Predictors in First-Ever Ischemic Stroke Patients: A Population-Based StudyFitri Amelia RizkiОценок пока нет
- Infection Control of Aerosol Transmissible DiseasesДокумент53 страницыInfection Control of Aerosol Transmissible DiseasesFitri Amelia RizkiОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Principles of General AnesthesiaДокумент60 страницPrinciples of General Anesthesiaمحمد عبد حسين100% (5)
- OKSIGENДокумент51 страницаOKSIGENlОценок пока нет
- S6 PowerPoint Videoconference Unit 4Документ26 страницS6 PowerPoint Videoconference Unit 4Jennifer Dariela Rivera MejiaОценок пока нет
- Assessment: Facial ShavingДокумент2 страницыAssessment: Facial ShavingA CОценок пока нет
- Antipartum Heamorrhage: Presenter Nsubuga Ivan MBCHB Stud 3.2 Kiu Lira Center Date 23 / 2 /2022Документ49 страницAntipartum Heamorrhage: Presenter Nsubuga Ivan MBCHB Stud 3.2 Kiu Lira Center Date 23 / 2 /2022Nsubuga IvanОценок пока нет
- Maya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewДокумент18 страницMaya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewsukmarahastriОценок пока нет
- Assessment 4 (BE)Документ9 страницAssessment 4 (BE)Aryan Judith DoloresОценок пока нет
- Abnormality PsychologyДокумент4 страницыAbnormality PsychologyYuen-Shan LeeОценок пока нет
- KAD Pada DM Tipe 1Документ56 страницKAD Pada DM Tipe 1hilmiana putriОценок пока нет
- Najlaa Exam 12-03-17Документ17 страницNajlaa Exam 12-03-17Abdul SalamОценок пока нет
- Rheumatic Heart Disease Abx Prophylaxis For Young PatientsДокумент2 страницыRheumatic Heart Disease Abx Prophylaxis For Young PatientsFathima Sheik KatherОценок пока нет
- HIV ManagmentДокумент44 страницыHIV ManagmentSarvesh PatilОценок пока нет
- CholesteatomaДокумент29 страницCholesteatomawhitelotusoo7Оценок пока нет
- Facial PalsyДокумент7 страницFacial PalsyPedro FonsecaОценок пока нет
- Aspirin (Acetyl-Salicylic Acid) Drug MonographДокумент1 страницаAspirin (Acetyl-Salicylic Acid) Drug MonographMuhammad Arsalan100% (1)
- 300+ TOP CASE MANAGER Objective Questions and AnswersДокумент29 страниц300+ TOP CASE MANAGER Objective Questions and AnswersHANEESH JOHNОценок пока нет
- Hypertensive CrisisДокумент28 страницHypertensive CrisisJacob Alexander MarpaungОценок пока нет
- 2.1 Market Analysis of Non-Needle Injector in IndonesiaДокумент5 страниц2.1 Market Analysis of Non-Needle Injector in IndonesiaPROFESSOR HUDAОценок пока нет
- Wellness CenterДокумент6 страницWellness CenterMuntasir SizanОценок пока нет
- Yellow Card LetterДокумент11 страницYellow Card LetterJamie White100% (6)
- FN-SSB 119Документ5 страницFN-SSB 119LunaPolidoОценок пока нет
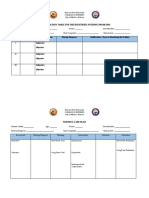
- Prioritization Table For The Identified Nursing ProblemsДокумент3 страницыPrioritization Table For The Identified Nursing ProblemsMia PascualОценок пока нет
- Running Head: REFLECTION ARTIFACT 1Документ21 страницаRunning Head: REFLECTION ARTIFACT 1api-396212664Оценок пока нет
- 3.1 Midwifery & Gynaecology Nursing Papers QPДокумент14 страниц3.1 Midwifery & Gynaecology Nursing Papers QPTapobrata Sarkar100% (1)
- De Juan, Joshua G. PE Q2 Module 6 Be Involved! Be Fit and Healthy!Документ6 страницDe Juan, Joshua G. PE Q2 Module 6 Be Involved! Be Fit and Healthy!Hanah Grace GomezОценок пока нет
- On Target - Ensuring Geometric Accuracy in Radiotherapy (2008, RCR)Документ76 страницOn Target - Ensuring Geometric Accuracy in Radiotherapy (2008, RCR)Milda InayahОценок пока нет
- Atrezia Coanala Este o Conditie Congenitala in Care Regiunea Posterioara A Pasajului Nazal (Coana) Este Blocata, de ObiceiДокумент5 страницAtrezia Coanala Este o Conditie Congenitala in Care Regiunea Posterioara A Pasajului Nazal (Coana) Este Blocata, de ObiceiTatiana NegrituОценок пока нет
- Sars-Cov-2 (Causative Agent of Covid-19) Viral Rna Detected (+)Документ1 страницаSars-Cov-2 (Causative Agent of Covid-19) Viral Rna Detected (+)Dominica PalacioОценок пока нет
- Small Renal MassДокумент26 страницSmall Renal MassSausan RasmiyyahОценок пока нет
- Case Study Part 2 Patient With Uti (Bag-O)Документ48 страницCase Study Part 2 Patient With Uti (Bag-O)Eaht Quirong0% (1)