Вам также может понравиться
- Broyd 2016Документ27 страницBroyd 2016Henry Leroy Lewis BatresОценок пока нет
- Changed Processing of Visual Sexual Stimuli Under GnRH-therapy - A Single Case Study in Pedophilia Using Eye Tracking and fMRIДокумент13 страницChanged Processing of Visual Sexual Stimuli Under GnRH-therapy - A Single Case Study in Pedophilia Using Eye Tracking and fMRIEmy Noviana SandyОценок пока нет
- Long-Term Stimulant Treatment Affects Brain Dopamine Transporter Level in Patients With Attention Deficit Hyperactive DisorderДокумент6 страницLong-Term Stimulant Treatment Affects Brain Dopamine Transporter Level in Patients With Attention Deficit Hyperactive DisorderpriyaОценок пока нет
- Modafinil For Cognitive NeuroenhancementДокумент35 страницModafinil For Cognitive NeuroenhancementAImeé MontoyaОценок пока нет
- Structural and Functional Imaging Studies in Chronic Cannabis Users - A Systematic Review of Adolescent and Adult FindingsДокумент1 страницаStructural and Functional Imaging Studies in Chronic Cannabis Users - A Systematic Review of Adolescent and Adult FindingsJ Alejandro ReyesОценок пока нет
- EtiologyДокумент3 страницыEtiologyapi-355875327Оценок пока нет
- Silveira 2016Документ61 страницаSilveira 2016Acupuntura de EquinosОценок пока нет
- Ecstasy Research PaperДокумент8 страницEcstasy Research Paperlyn0l1gamop2100% (1)
- Understanding Drug Abuse and Addiction What Science Says PDFДокумент32 страницыUnderstanding Drug Abuse and Addiction What Science Says PDFAljen CastilloОценок пока нет
- 0-Addicto Craving Hone-Blanchet (2014)Документ15 страниц0-Addicto Craving Hone-Blanchet (2014)gildas5d5almeidaОценок пока нет
- Long-Term Effects of Marijuana Use On The Brain: A B C DДокумент6 страницLong-Term Effects of Marijuana Use On The Brain: A B C DgabhekОценок пока нет
- 4-Effects of Different Combined Behavioral and Pharmacological Interventions On Smoking Cessation A Network Meta-Analysis of 103 Randomized Controlled TrialsДокумент11 страниц4-Effects of Different Combined Behavioral and Pharmacological Interventions On Smoking Cessation A Network Meta-Analysis of 103 Randomized Controlled Trialszhouliying684Оценок пока нет
- Mary 2Документ38 страницMary 2Bernard DarkwahОценок пока нет
- Artigo NFD Efficacy of Invasive and Non-Invasive Brain ModulationДокумент23 страницыArtigo NFD Efficacy of Invasive and Non-Invasive Brain ModulationMarcelo MenezesОценок пока нет
- Non-Medical Use of Illicit DrugsДокумент209 страницNon-Medical Use of Illicit DrugsChemistixОценок пока нет
- 06 - Addiction Conceptual - With TanviДокумент8 страниц06 - Addiction Conceptual - With TanviSarita KapgateОценок пока нет
- KKDK Aquinobete FinalsДокумент22 страницыKKDK Aquinobete FinalsAngela Magpantay PeОценок пока нет
- EBSCO FullText 2023 08 16 1Документ11 страницEBSCO FullText 2023 08 16 1PaulОценок пока нет
- Volkow 2018Документ12 страницVolkow 2018Marcos AlexandreОценок пока нет
- Anti Colin Erg I CosДокумент19 страницAnti Colin Erg I CosCentro De Salud PrevenirОценок пока нет
- Preoperative Interventions For Alcohol and Other Recreational Substance Use: A Systematic Review and Meta-AnalysisДокумент18 страницPreoperative Interventions For Alcohol and Other Recreational Substance Use: A Systematic Review and Meta-AnalysiscecileОценок пока нет
- Illicit Drug Use in Cluster Headache Patients and in The General Population: A Comparative Cross-Sectional SurveyДокумент10 страницIllicit Drug Use in Cluster Headache Patients and in The General Population: A Comparative Cross-Sectional SurveyRicky HerdiantoОценок пока нет
- Metabolites 10 00072Документ20 страницMetabolites 10 00072joseph psychayterОценок пока нет
- AlcoholДокумент16 страницAlcoholAna Maria BuenoОценок пока нет
- A Case-Comparison Study of Executive Functions in Alcohol-Dependent Adults With Maternal History of AlcoholismДокумент6 страницA Case-Comparison Study of Executive Functions in Alcohol-Dependent Adults With Maternal History of AlcoholismmirymirelaОценок пока нет
- Substance Use and Recidivism Outcomes For Prison-Based Drug and Alcohol Interventions-FinalДокумент19 страницSubstance Use and Recidivism Outcomes For Prison-Based Drug and Alcohol Interventions-FinalFelix Omondi SceneryОценок пока нет
- Grant Neurocognitive Effects of Cannabis JINS 2003Документ11 страницGrant Neurocognitive Effects of Cannabis JINS 2003sarysulastioОценок пока нет
- Chen2017 - Similarities and Differences in PsychologyДокумент11 страницChen2017 - Similarities and Differences in Psychologyhilda.marselaОценок пока нет
- Ehrenrich Et - Al. 99Документ30 страницEhrenrich Et - Al. 99Матиас Себальос ГусманОценок пока нет
- Mark Mclaughlin Annotated Bibliography 1Документ8 страницMark Mclaughlin Annotated Bibliography 1api-625527319Оценок пока нет
- Cannabis Sixteen Countries 2021Документ14 страницCannabis Sixteen Countries 2021Alfredo MorenoОценок пока нет
- MarfaGil Cristina PRC2 CATДокумент17 страницMarfaGil Cristina PRC2 CATCristina Marfa GilОценок пока нет
- So Boka 2017Документ7 страницSo Boka 2017Kurnia pralisaОценок пока нет
- Donadon Et Al, 2014 - AlcoolismoДокумент9 страницDonadon Et Al, 2014 - Alcoolismoroselita321Оценок пока нет
- Medicina 56 00453Документ3 страницыMedicina 56 00453Michael UОценок пока нет
- Neuropsychophysiological Measures of Alcohol Dependence: Can We Use EEG in The Clinical Assessment?Документ17 страницNeuropsychophysiological Measures of Alcohol Dependence: Can We Use EEG in The Clinical Assessment?DianaLunguОценок пока нет
- Neuromodulation For Addiction 082209Документ9 страницNeuromodulation For Addiction 082209hellno1234100% (1)
- Chapter 2 NeurobiologyДокумент31 страницаChapter 2 Neurobiologyanitha1118Оценок пока нет
- Drugs and The BrainДокумент6 страницDrugs and The BrainSherryl PontillasОценок пока нет
- Fernandez Serrano2009Документ17 страницFernandez Serrano2009Dilan GutierrezОценок пока нет
- Treating Drug Dependence With The Aid of Ibogaine: A Qualitative StudyДокумент10 страницTreating Drug Dependence With The Aid of Ibogaine: A Qualitative StudyeduardoschenbergОценок пока нет
- Marijuana Effects On Human BrainДокумент5 страницMarijuana Effects On Human BrainKashMalhotraОценок пока нет
- Effects of Modafiil and Bromazepam On Decision-Making: A P300 AnalysisДокумент13 страницEffects of Modafiil and Bromazepam On Decision-Making: A P300 AnalysisInternational Medical PublisherОценок пока нет
- Smoke Cessation 1Документ15 страницSmoke Cessation 1Ricardo GalhardoniОценок пока нет
- Diana, 2018Документ14 страницDiana, 2018Ale López CastroОценок пока нет
- Outcome - Predictors - in - Substance - Use - DisoДокумент29 страницOutcome - Predictors - in - Substance - Use - Disoalexandra mariaОценок пока нет
- PNAS-cannabis UsersДокумент8 страницPNAS-cannabis UsersPriscila Previato de AlmeidaОценок пока нет
- Hormonal Response in GamblingДокумент23 страницыHormonal Response in GamblingMihaelaSiVictoriaОценок пока нет
- Adiksi Prof PDF Bab 8Документ28 страницAdiksi Prof PDF Bab 8tito syahjihadОценок пока нет
- EuropeanResponsesGuide2017 - BackgroundPaper Evidence Review Drug InterventionsДокумент25 страницEuropeanResponsesGuide2017 - BackgroundPaper Evidence Review Drug InterventionsAnkit ShahiОценок пока нет
- 2014 Article 35 PDFДокумент10 страниц2014 Article 35 PDFLena Wahyu SetianingsihОценок пока нет
- Effectiveness of Dynamic Homoeopathic Preparation of Dependent SubjectsДокумент4 страницыEffectiveness of Dynamic Homoeopathic Preparation of Dependent SubjectsVarshaОценок пока нет
- 1 s2.0 S0079612315001909 MainДокумент27 страниц1 s2.0 S0079612315001909 Mainqnx22605Оценок пока нет
- CV Vivek Benegal 0610Документ16 страницCV Vivek Benegal 0610bhaskarsg0% (1)
- Conducere Sub Influenta AlcooluluiДокумент6 страницConducere Sub Influenta Alcooluluioana_roxana2005stОценок пока нет
- Calidad de Vida 03Документ7 страницCalidad de Vida 03RosarioBengocheaSecoОценок пока нет
- tmpA58E TMPДокумент8 страницtmpA58E TMPFrontiersОценок пока нет
- International Encylopedia of Social Behavioral Sciences PDFДокумент222 страницыInternational Encylopedia of Social Behavioral Sciences PDFVi KekaОценок пока нет
- APA - DSM 5 Internet Gaming Disorder PDFДокумент1 страницаAPA - DSM 5 Internet Gaming Disorder PDFcristina05Оценок пока нет
- About Villa 21 David CooperДокумент13 страницAbout Villa 21 David CooperVi KekaОценок пока нет
- How To Make A Country HamДокумент9 страницHow To Make A Country HamVi KekaОценок пока нет
- Autistic Traits in The General Population: A Twin StudyДокумент7 страницAutistic Traits in The General Population: A Twin StudyVi KekaОценок пока нет
- Artykul NLPДокумент9 страницArtykul NLPAnna ZipperОценок пока нет
- Bond Deception - Detection - Expertise PDFДокумент13 страницBond Deception - Detection - Expertise PDFVi KekaОценок пока нет
- Beginner's Guide To BJJДокумент56 страницBeginner's Guide To BJJVi Keka100% (9)
- Part I and II - The Historical MujushinДокумент6 страницPart I and II - The Historical MujushinVi Keka100% (2)
- About Villa 21 David CooperДокумент13 страницAbout Villa 21 David CooperVi KekaОценок пока нет
- The Wrath of OdinДокумент1 страницаThe Wrath of OdinVi KekaОценок пока нет
- Cinnamon RollДокумент2 страницыCinnamon RollVi KekaОценок пока нет
- Artykul NLPДокумент9 страницArtykul NLPAnna ZipperОценок пока нет
- PsicopatologiaДокумент109 страницPsicopatologiaVi KekaОценок пока нет
- The Social Animal Aronson PDFДокумент40 страницThe Social Animal Aronson PDFNiky Papuc67% (9)
- Part III - The Mujuushin in Samurai Champloo - Sword of No Abiding MindДокумент4 страницыPart III - The Mujuushin in Samurai Champloo - Sword of No Abiding MindVi KekaОценок пока нет
- Japanese SwordДокумент32 страницыJapanese SwordGrimm CaoОценок пока нет
- EC Multiple Intelligences RevisitedДокумент114 страницEC Multiple Intelligences RevisitedDrAmira El-amir KhaterОценок пока нет
- 18135Документ13 страниц18135Rofi' Serin Ve AkilliОценок пока нет
- Exploratory Factor Analysis Kootstra 04Документ15 страницExploratory Factor Analysis Kootstra 04Vi KekaОценок пока нет
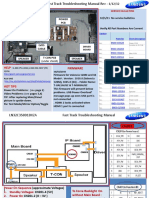
- Samsung LN55C610N1FXZA Fast Track Guide (SM)Документ4 страницыSamsung LN55C610N1FXZA Fast Track Guide (SM)Carlos OdilonОценок пока нет
- Blackrock Methods of Delay AnalysisДокумент36 страницBlackrock Methods of Delay AnalysisAhmed MoubarkОценок пока нет
- Recovering The Snorra Edda On Playing Gods, Loki, and The Importance of HistoryДокумент17 страницRecovering The Snorra Edda On Playing Gods, Loki, and The Importance of HistoryM SОценок пока нет
- Position Trading Maximizing Probability of Winning TradesДокумент91 страницаPosition Trading Maximizing Probability of Winning Tradescarlo bakaakoОценок пока нет
- PGT Computer Science Kendriya Vidyalaya Entrance Exam Question PapersДокумент117 страницPGT Computer Science Kendriya Vidyalaya Entrance Exam Question PapersimshwezОценок пока нет
- Al Rafay ProfileДокумент8 страницAl Rafay ProfileRana UsmanОценок пока нет
- CIVIL 3811 - Lecture Slides - Week 7Документ58 страницCIVIL 3811 - Lecture Slides - Week 7hadaОценок пока нет
- Elaborare Modele de Rating in Conformitate Cu IFRS 9Документ8 страницElaborare Modele de Rating in Conformitate Cu IFRS 9MstefОценок пока нет
- ScriptДокумент12 страницScriptWaleed Nadeem50% (2)
- Gunnar Fischer's Work On Ingmar Bergman's The Seventh Seal and Wild StrawberriesДокумент6 страницGunnar Fischer's Work On Ingmar Bergman's The Seventh Seal and Wild StrawberriesSaso Dimoski100% (1)
- Pyrethroids April 11Документ15 страницPyrethroids April 11MadhumithaОценок пока нет
- FPA 03-A.01 Permohonan Akreditasi LP LK LI LM PUP PBAДокумент595 страницFPA 03-A.01 Permohonan Akreditasi LP LK LI LM PUP PBAabimanyubawonoОценок пока нет
- Unpriced Proposed Renovation of Bugolobi Flat, Block C For Uganda Coffee Development AuthorityДокумент39 страницUnpriced Proposed Renovation of Bugolobi Flat, Block C For Uganda Coffee Development AuthoritynicolasОценок пока нет
- Durham E-ThesesДокумент203 страницыDurham E-ThesesH Man SharifОценок пока нет
- Annex 1: Homeroom Guidance Monitoring Tool (School Level) Homeroom Guidance Monitoring ToolДокумент2 страницыAnnex 1: Homeroom Guidance Monitoring Tool (School Level) Homeroom Guidance Monitoring ToolMariel Gregore0% (1)
- MGMT 4Документ26 страницMGMT 4Said GunayОценок пока нет
- B - ELSB - Cat - 2020 PDFДокумент850 страницB - ELSB - Cat - 2020 PDFanupamОценок пока нет
- What Is StevedoringДокумент10 страницWhat Is StevedoringMinhaj KmОценок пока нет
- New Life in Christ - Vol05 - Engl - Teacher GuideДокумент29 страницNew Life in Christ - Vol05 - Engl - Teacher GuideOliver Angus100% (1)
- Tabulation Sheet (LABO)Документ9 страницTabulation Sheet (LABO)KetIanCotalesОценок пока нет
- Sheiko 13week Beginner ProgramДокумент16 страницSheiko 13week Beginner ProgramAnders DahlОценок пока нет
- Can J Chem Eng - 2022 - Mocellin - Experimental Methods in Chemical Engineering Hazard and Operability Analysis HAZOPДокумент20 страницCan J Chem Eng - 2022 - Mocellin - Experimental Methods in Chemical Engineering Hazard and Operability Analysis HAZOPbademmaliОценок пока нет
- Method For Determination of Iron Folic Acid & Vitamin B12 in FRK - 07.11.2023Документ17 страницMethod For Determination of Iron Folic Acid & Vitamin B12 in FRK - 07.11.2023jonesbennetteОценок пока нет
- Power Factor Improvement SystemДокумент25 страницPower Factor Improvement SystemBijoy SahaОценок пока нет
- Emc VNX MatrixДокумент8 страницEmc VNX Matrixpolivni0% (1)
- Central Venous PressureДокумент3 страницыCentral Venous PressureHuy NguyễnОценок пока нет
- Tuan Nor Akmal Imanina Binti Tuan MasorДокумент2 страницыTuan Nor Akmal Imanina Binti Tuan MasorIzza RosliОценок пока нет
- Sector San Juan Guidance For RepoweringДокумент12 страницSector San Juan Guidance For RepoweringTroy IveyОценок пока нет
- Olp Lesson PlanДокумент2 страницыOlp Lesson Planapi-654865620Оценок пока нет
- 2010 DOE FEMP Exterior Lighting GuideДокумент38 страниц2010 DOE FEMP Exterior Lighting GuideMoideen Thashreef100% (1)