Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Low Back Pain PDFДокумент4 страницыLow Back Pain PDFnetifarhatiiОценок пока нет
- Cerebral Palsy JurnalДокумент17 страницCerebral Palsy JurnaltrieОценок пока нет
- Research ArticleДокумент13 страницResearch ArticlenetifarhatiiОценок пока нет
- En A11v14n5 PDFДокумент9 страницEn A11v14n5 PDFnetifarhatiiОценок пока нет
- Thorax 2010 Chapman 747 52 PDFДокумент7 страницThorax 2010 Chapman 747 52 PDFnetifarhatiiОценок пока нет
- Indian Journal of Tuberculosis - Volume 57 - No.1 Jan-2010 PDFДокумент62 страницыIndian Journal of Tuberculosis - Volume 57 - No.1 Jan-2010 PDFnetifarhatiiОценок пока нет
- Diagnosis and Management of Myasthenia Gravis: ReviewДокумент9 страницDiagnosis and Management of Myasthenia Gravis: ReviewnetifarhatiiОценок пока нет
- Kjo 25 1Документ7 страницKjo 25 1netifarhatiiОценок пока нет
- The World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines For The Biological Treatment of ParaphiliasДокумент52 страницыThe World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines For The Biological Treatment of ParaphiliasanhiramdhaniОценок пока нет
- Lumbar Radicular Pain: PathophysiologyДокумент4 страницыLumbar Radicular Pain: PathophysiologynetifarhatiiОценок пока нет
- VertigoДокумент19 страницVertigonetifarhatiiОценок пока нет
- EpilepsyДокумент38 страницEpilepsyJareena BegumОценок пока нет
- Pseudofollicular BabaeДокумент13 страницPseudofollicular BabaeOlamide EstherОценок пока нет
- ARES Protocol Os UseДокумент5 страницARES Protocol Os UseLeia AlbaОценок пока нет
- Suicide in Adolescent - A Case ReportДокумент5 страницSuicide in Adolescent - A Case ReportRebecca SilaenОценок пока нет
- Systemic Diseases and The EyeДокумент17 страницSystemic Diseases and The Eyeapi-337689057Оценок пока нет
- Preeclampsia Nursing Care PlanДокумент5 страницPreeclampsia Nursing Care PlanBSN 3-2 RUIZ, Jewel Anne F.Оценок пока нет
- Subinvolution Breast Complications: Prepared by Ms. Annu Panchal Assistant ProfessorДокумент19 страницSubinvolution Breast Complications: Prepared by Ms. Annu Panchal Assistant Professorannu panchalОценок пока нет
- Immnunology Notebook Chapter One: Innate ImmunityДокумент45 страницImmnunology Notebook Chapter One: Innate ImmunityJavier Alejandro Daza GalvánОценок пока нет
- LESSON 3: Exercise Variables and PrinciplesДокумент31 страницаLESSON 3: Exercise Variables and PrinciplesCapulong Kimberly100% (1)
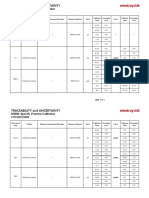
- Specific Proteins Calibrator-150721009-BS600Документ2 страницыSpecific Proteins Calibrator-150721009-BS600S6b2Оценок пока нет
- Anxiety: What Are Some Symptoms of Anxiety?Документ3 страницыAnxiety: What Are Some Symptoms of Anxiety?Khairil AshrafОценок пока нет
- Insights and Images: Vascular Channel Mimicking A Skull FractureДокумент2 страницыInsights and Images: Vascular Channel Mimicking A Skull Fracturethariq mubarakОценок пока нет
- AQ4PДокумент3 страницыAQ4PAhmed GaberОценок пока нет
- New Health Care Clinical: Laboratory SrinagarДокумент1 страницаNew Health Care Clinical: Laboratory SrinagarRajaОценок пока нет
- SeizureДокумент10 страницSeizureRomeo ReyesОценок пока нет
- Modifiers-Table 122015 2Документ25 страницModifiers-Table 122015 2khatОценок пока нет
- An Unconscious Patient With A DNR TattooДокумент2 страницыAn Unconscious Patient With A DNR TattoonadaОценок пока нет
- +++A Short Survey in Application of Ordinary Differential Equations On Cancer ResearchДокумент5 страниц+++A Short Survey in Application of Ordinary Differential Equations On Cancer ResearchEnes ÇakmakОценок пока нет
- Allergic Contact DermatitisДокумент12 страницAllergic Contact DermatitisAzis BoenjaminОценок пока нет
- Anesthesia-Assessing Depth PDFДокумент1 страницаAnesthesia-Assessing Depth PDFAvinash Technical ServiceОценок пока нет
- Infusion PumpДокумент14 страницInfusion PumpSREEDEVI T SURESHОценок пока нет
- Evaluation of Bacterial Agents Isolated From Aspirate Cultures of Covid 19 General Intensivecare Patients Compared To Pre Pandemic ConditionsДокумент8 страницEvaluation of Bacterial Agents Isolated From Aspirate Cultures of Covid 19 General Intensivecare Patients Compared To Pre Pandemic ConditionsRicardo ZúñigaОценок пока нет
- He2011 TMJ ANKYLOSIS CLASSIFICATIONДокумент8 страницHe2011 TMJ ANKYLOSIS CLASSIFICATIONPorcupine TreeОценок пока нет
- Detoxification:Management of AmaДокумент3 страницыDetoxification:Management of AmaqueencelОценок пока нет
- On and Off Male Birth Control MethodsДокумент2 страницыOn and Off Male Birth Control MethodsLeón L.PОценок пока нет
- Celiac DiseaseДокумент35 страницCeliac DiseaseRye HanaОценок пока нет
- Massage Techniques and Effects PresentationДокумент35 страницMassage Techniques and Effects Presentationama00Оценок пока нет
- PMLSДокумент9 страницPMLSChan ChanОценок пока нет
- Ok - Effect of Melatonin On Broiler ChicksДокумент12 страницOk - Effect of Melatonin On Broiler ChicksOliver TalipОценок пока нет
- Wards and Departments in The Hospital NamingДокумент4 страницыWards and Departments in The Hospital NamingSlebeww PetewОценок пока нет