Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Design of Water Supply System-High Rise BLDGДокумент108 страницDesign of Water Supply System-High Rise BLDGcris bunagОценок пока нет
- Processing of Synthetic Aperture Radar Images - H. Maitre (Wiley, 2008) WWДокумент411 страницProcessing of Synthetic Aperture Radar Images - H. Maitre (Wiley, 2008) WWbehzad100% (4)
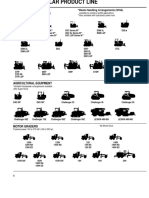
- Caterpillar Product Line 13Документ7 страницCaterpillar Product Line 13GenneraalОценок пока нет
- ABC of Liver Pancreas and Gall BladderДокумент65 страницABC of Liver Pancreas and Gall BladderMayer Rosenberg100% (3)
- Hazardous Area ClassificationДокумент36 страницHazardous Area Classificationvenkeeku100% (1)
- Elecon GearboxДокумент19 страницElecon GearboxShirley Farrace100% (3)
- 00.concrete Mix Design-RailwayДокумент38 страниц00.concrete Mix Design-RailwaySoundar PachiappanОценок пока нет
- Elementary Surveying Problem Set 2 q1Документ2 страницыElementary Surveying Problem Set 2 q1soontobengineer50% (2)
- Hungarian NotationДокумент6 страницHungarian NotationmelpaniОценок пока нет
- Abdominal X Rays Made Easy - Abnormal Intraluminal GasДокумент2 страницыAbdominal X Rays Made Easy - Abnormal Intraluminal GasRodry Mikhael Lumban TobingОценок пока нет
- Axr Easy 1Документ2 страницыAxr Easy 1aboelfotohbadrОценок пока нет
- 2007 Human Behavior Course Block 3 ExamДокумент11 страниц2007 Human Behavior Course Block 3 Exam128551986Оценок пока нет
- 2nd LecДокумент15 страниц2nd Lec128551986Оценок пока нет
- PR100 BrochureДокумент28 страницPR100 Brochuregus289Оценок пока нет
- Sti260N6F6 Stp260N6F6: N-Channel 60 V, 0.0024 Ω, 120 A Stripfet™ Vi Deepgate™ Power Mosfet In To-220 And I²Pak PackagesДокумент14 страницSti260N6F6 Stp260N6F6: N-Channel 60 V, 0.0024 Ω, 120 A Stripfet™ Vi Deepgate™ Power Mosfet In To-220 And I²Pak PackagesRyn YahuFОценок пока нет
- (Frankel 1962) The Production Function in Allocation and GrowthДокумент29 страниц(Frankel 1962) The Production Function in Allocation and GrowthT-roy Taylor100% (1)
- Ijarece Vol 8 Issue 8 141 144Документ4 страницыIjarece Vol 8 Issue 8 141 144Rnav rnavОценок пока нет
- Assignment - 1 Introduction of Machines and Mechanisms: TheoryДокумент23 страницыAssignment - 1 Introduction of Machines and Mechanisms: TheoryAman AmanОценок пока нет
- Lab Manual of Hydraulics PDFДокумент40 страницLab Manual of Hydraulics PDFJULIUS CESAR G. CADAOОценок пока нет
- Downloadble Science NotesДокумент55 страницDownloadble Science NotesJeb PampliegaОценок пока нет
- FP - ES - 28 - Rindu Grahabhakti Intani - PERMEABLE ENTRY CHARACTERIZATION AT DARAJAT FIELD, WEST JAVA PDFДокумент4 страницыFP - ES - 28 - Rindu Grahabhakti Intani - PERMEABLE ENTRY CHARACTERIZATION AT DARAJAT FIELD, WEST JAVA PDFrindu_intaniОценок пока нет
- Comptector & Chiller (Cdu) Controller (Fx32C Series) : Precaution For UseДокумент5 страницComptector & Chiller (Cdu) Controller (Fx32C Series) : Precaution For UseFcma0903100% (1)
- IFoA Directory of Actuarial Employers 2016-17-14102016Документ22 страницыIFoA Directory of Actuarial Employers 2016-17-14102016Mian BialОценок пока нет
- Semi Conductors: The Start of Information AgeДокумент15 страницSemi Conductors: The Start of Information AgeMarvin LabajoОценок пока нет
- Frequency AdverbsДокумент4 страницыFrequency AdverbsAlexander ScrОценок пока нет
- XG5000 Manual (2009.10.26) (Eng)Документ645 страницXG5000 Manual (2009.10.26) (Eng)wanderly_40100% (1)
- 8 Coil PWM Drivers PDFДокумент4 страницы8 Coil PWM Drivers PDFDuzng Hoang TriОценок пока нет
- Permability & Seepage-Dr Siddharth G Shah PDFДокумент8 страницPermability & Seepage-Dr Siddharth G Shah PDFSG ShahОценок пока нет
- G3412 - 450 KW Performance DataДокумент3 страницыG3412 - 450 KW Performance DataJacob De CasillasОценок пока нет
- Organic Chemistry - Some Basic Principles and Techniques-1Документ195 страницOrganic Chemistry - Some Basic Principles and Techniques-1aditya kumar Agarwal100% (1)
- Real Time Operating SystemsДокумент15 страницReal Time Operating SystemsSaro VrsОценок пока нет
- Customer DemandДокумент42 страницыCustomer Demandtulika_ajwaniОценок пока нет
- Research and Development at The BENSON Test RigДокумент20 страницResearch and Development at The BENSON Test RigsbktceОценок пока нет
- Surface Mount Multilayer Varistor: SC0805ML - SC2220ML SeriesДокумент8 страницSurface Mount Multilayer Varistor: SC0805ML - SC2220ML SeriesTalebОценок пока нет
- NumaticsFRLFlexiblokR072010 EsДокумент40 страницNumaticsFRLFlexiblokR072010 EsGabriel San Martin RifoОценок пока нет