Вам также может понравиться
- Allen2009 PDFДокумент8 страницAllen2009 PDFJack ButcherОценок пока нет
- Neumonia AspirativaДокумент11 страницNeumonia AspirativaJack ButcherОценок пока нет
- Alcohol Alcohol Algodon Algodon Algodon L AlgodonДокумент1 страницаAlcohol Alcohol Algodon Algodon Algodon L AlgodonJack ButcherОценок пока нет
- Neumonia AspirativaДокумент11 страницNeumonia AspirativaJack ButcherОценок пока нет
- Clinical CasesДокумент183 страницыClinical Casesdaisyputih80% (5)
- Clinical CasesДокумент183 страницыClinical Casesdaisyputih80% (5)
- Bouch Lario To U 2014 GGGДокумент7 страницBouch Lario To U 2014 GGGJack ButcherОценок пока нет
- AbruptionДокумент12 страницAbruptionAdhy PallyОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Mullā Ṣadrā and Causation - Rethinking A Problem in Later Islamic Philosophy AuthorДокумент15 страницMullā Ṣadrā and Causation - Rethinking A Problem in Later Islamic Philosophy AuthorKadag LhundrupОценок пока нет
- Fret Position Calculator - StewmacДокумент1 страницаFret Position Calculator - StewmacJuan Pablo Sepulveda SierraОценок пока нет
- Latihan To: Nilai: 7.4 Benar: 37 Salah: 13Документ17 страницLatihan To: Nilai: 7.4 Benar: 37 Salah: 13glensОценок пока нет
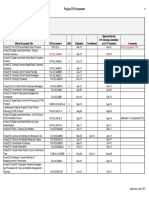
- Approved Project 25 StandardsДокумент5 страницApproved Project 25 StandardsepidavriosОценок пока нет
- Understanding Bernoulli's Principle Through Simulations PDFДокумент4 страницыUnderstanding Bernoulli's Principle Through Simulations PDFIoannis GaroufalidisОценок пока нет
- Iron Ore ProcessДокумент52 страницыIron Ore Processjafary448067% (3)
- Exercise 9 Two Factor Factorial Experiments and Derivation of Expected Mean SquaresДокумент14 страницExercise 9 Two Factor Factorial Experiments and Derivation of Expected Mean SquaresHasmaye PintoОценок пока нет
- Relationsh Between EM and Young S ModuliДокумент7 страницRelationsh Between EM and Young S ModuliDwight AndersonОценок пока нет
- DCS YokogawaДокумент17 страницDCS Yokogawasswahyudi100% (1)
- Cell Wall Synthesis InhibitorsДокумент6 страницCell Wall Synthesis InhibitorsRPh Krishna Chandra JagritОценок пока нет
- Generalized Anxiety DisorderДокумент24 страницыGeneralized Anxiety DisorderEula Angelica OcoОценок пока нет
- A Presentation On-: Dr. Nikhil Oza Intern BvdumcДокумент43 страницыA Presentation On-: Dr. Nikhil Oza Intern BvdumcMaheboob GanjalОценок пока нет
- BS746 2014Документ22 страницыBS746 2014marco SimonelliОценок пока нет
- Communication Models in Internet of Things: A SurveyДокумент5 страницCommunication Models in Internet of Things: A SurveyIJSTEОценок пока нет
- VTA28-G5: Fuel OptimizedДокумент3 страницыVTA28-G5: Fuel OptimizedIslam HemdanОценок пока нет
- Overall Method StatementДокумент33 страницыOverall Method Statementsaranga100% (1)
- Sheet Metal Manufacturing Companies NoidaДокумент9 страницSheet Metal Manufacturing Companies NoidaAmanda HoldenОценок пока нет
- Five Star Hotel and ResortДокумент9 страницFive Star Hotel and ResortAISHОценок пока нет
- Abdominal Examination OSCE GuideДокумент30 страницAbdominal Examination OSCE Guideزياد سعيدОценок пока нет
- Tesla Magazine Vol4Документ48 страницTesla Magazine Vol4jonathan100% (1)
- Paranoia XP - Gamemaster Screen Booklet - Mandatory Fun Enforcement PackДокумент24 страницыParanoia XP - Gamemaster Screen Booklet - Mandatory Fun Enforcement PackStBash100% (3)
- Tsel Manual ThermoselДокумент25 страницTsel Manual ThermoselPedro AlvelaisОценок пока нет
- PEДокумент12 страницPEMae Ann Base RicafortОценок пока нет
- Motor CAT C13 AcertДокумент3 страницыMotor CAT C13 AcertJosé Gonzalez100% (4)
- Marvell 88F37xx Product Brief 20160830Документ2 страницыMarvell 88F37xx Product Brief 20160830Sassy FiverОценок пока нет
- Navy Supplement To The DOD Dictionary of Military and Associated Terms, 2011Документ405 страницNavy Supplement To The DOD Dictionary of Military and Associated Terms, 2011bateljupko100% (1)
- Aluminium Alloy - Wikipedia, The Free EncyclopediaДокумент12 страницAluminium Alloy - Wikipedia, The Free EncyclopediaAshishJoshi100% (1)
- 09.tracheostomy Management by Speech Language Pathologists in SwedenДокумент12 страниц09.tracheostomy Management by Speech Language Pathologists in SwedenCarlonchaCáceresОценок пока нет
- Zest O CorporationДокумент21 страницаZest O CorporationJhamane Chan53% (15)
- LPPДокумент4 страницыLPPMargarida ReisОценок пока нет