Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Fundamental of PhysiotherapyДокумент142 страницыFundamental of PhysiotherapyFareeha Makhdoom100% (4)
- General Format For Orthopedic AssessmentДокумент27 страницGeneral Format For Orthopedic AssessmentMegha Patani100% (7)
- Provide Body Electrotherapy TreatmentsДокумент22 страницыProvide Body Electrotherapy Treatmentsebook100% (1)
- Sitbat 16item FinalДокумент6 страницSitbat 16item FinalMae NocheОценок пока нет
- Crawling Exercise: Dr. Hiral Katakia MPT (Neuro)Документ20 страницCrawling Exercise: Dr. Hiral Katakia MPT (Neuro)Rohan LAl100% (3)
- Bagua Rolling Step MethodДокумент4 страницыBagua Rolling Step MethodRamon CastellanosОценок пока нет
- Badminton Coaching 2016Документ32 страницыBadminton Coaching 2016dennis sabornidoОценок пока нет
- Dossier RPG EnglishДокумент15 страницDossier RPG EnglishtetevoОценок пока нет
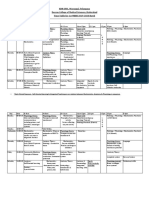
- KNRUHS 1st MBBS Time Table 2019-2020 DCMS - CumulativeДокумент42 страницыKNRUHS 1st MBBS Time Table 2019-2020 DCMS - CumulativeAnime FanОценок пока нет
- Unit 7: Anatomy: Excerpt From A LectureДокумент4 страницыUnit 7: Anatomy: Excerpt From A LectureAnonymous Wfl201YbYoОценок пока нет
- Wheelchair Curling Classification RulesДокумент9 страницWheelchair Curling Classification RulesIoan-Alexandru CodarceaОценок пока нет
- MOINA 1st SEM 1 1Документ14 страницMOINA 1st SEM 1 1Zach DemontanoОценок пока нет
- Traumatic Hip Dislocation in Children: Original StudyДокумент6 страницTraumatic Hip Dislocation in Children: Original StudyAlvin JiwonoОценок пока нет
- Neurological Examination of The Limbs TextДокумент8 страницNeurological Examination of The Limbs Textvidur_talrejaОценок пока нет
- Jis B 9708 e 2002Документ10 страницJis B 9708 e 2002josephkirbyОценок пока нет
- International Olympic Committee ConsensusДокумент18 страницInternational Olympic Committee ConsensusGabriella CananОценок пока нет
- NCP 2Документ3 страницыNCP 2klawdin100% (1)
- Posterior Abdominal WallДокумент125 страницPosterior Abdominal Wallarjun.k5796Оценок пока нет
- Sensorimotor Training A Global Approach For BalancДокумент9 страницSensorimotor Training A Global Approach For BalancVizaОценок пока нет
- '07 Sullivan CДокумент32 страницы'07 Sullivan CGeo NavarroОценок пока нет
- Copy p1 Week 5 Nur 098 ActivityДокумент5 страницCopy p1 Week 5 Nur 098 ActivityRomelyn DellezoОценок пока нет
- Hot Topics 6 MonthsДокумент2 страницыHot Topics 6 MonthsclarafranОценок пока нет
- 15 Head Neck Back Spine TMJ (Special Tests) (FINAL)Документ8 страниц15 Head Neck Back Spine TMJ (Special Tests) (FINAL)kath-kathОценок пока нет
- Describe Gross Anatomy of Axilla, Under The Following HeadingДокумент11 страницDescribe Gross Anatomy of Axilla, Under The Following HeadingOluwatobi EzekielОценок пока нет
- Positioning and Draping ChecklistДокумент5 страницPositioning and Draping ChecklistSean HolarОценок пока нет
- Anat MuscleДокумент164 страницыAnat Musclejohn delaОценок пока нет
- Balance Training in Hemiplegic PatientsДокумент9 страницBalance Training in Hemiplegic Patientsshobhna mishraОценок пока нет
- Quantifying The Functional Rehabilitation of Injured Football PlayersДокумент7 страницQuantifying The Functional Rehabilitation of Injured Football PlayersAmanda TuckerОценок пока нет
- Rolling NAJSPTДокумент13 страницRolling NAJSPTDiego LacerdaОценок пока нет
- Sindrome KompartemenДокумент1 страницаSindrome KompartemennurulОценок пока нет