Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
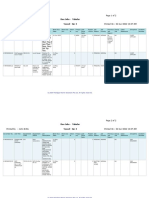
- Page 1 of 2: Due Jobs - Tabular Vessel - Arc IДокумент2 страницыPage 1 of 2: Due Jobs - Tabular Vessel - Arc IJohn MithuОценок пока нет
- Arenza Dry Dock ReportДокумент43 страницыArenza Dry Dock ReportJohn MithuОценок пока нет
- Defect List: Gas ArmaДокумент4 страницыDefect List: Gas ArmaJohn MithuОценок пока нет
- Details of MotorДокумент8 страницDetails of MotorJohn MithuОценок пока нет
- Campaign - Motor FailureДокумент13 страницCampaign - Motor FailureJohn MithuОценок пока нет
- Naturelle S2 Wire Rope Lubricant A TDSДокумент2 страницыNaturelle S2 Wire Rope Lubricant A TDSJohn MithuОценок пока нет
- TNPSC Group 4 2014 Question Paper - General English - WWW - Tnpscguru.inДокумент14 страницTNPSC Group 4 2014 Question Paper - General English - WWW - Tnpscguru.inJohn MithuОценок пока нет
- Get FilejhДокумент9 страницGet FilejhJohn MithuОценок пока нет
- Function: Controlling The Operation of The Ship & Care For Persons On Board at Management LevelДокумент3 страницыFunction: Controlling The Operation of The Ship & Care For Persons On Board at Management LevelJohn MithuОценок пока нет
- Budget For MBC: Crew Wages 2,460,000 Victuals 110,000 Other Crew Cost 200,000Документ2 страницыBudget For MBC: Crew Wages 2,460,000 Victuals 110,000 Other Crew Cost 200,000John MithuОценок пока нет
- AntifoulingДокумент3 страницыAntifoulingJohn MithuОценок пока нет
- STCWДокумент37 страницSTCWJohn Mithu80% (5)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Ambulatory CareДокумент11 страницAmbulatory Caremitishahirlekar100% (1)
- Architect Plan For Rainbow VistasДокумент3 страницыArchitect Plan For Rainbow Vistassaikrishna padarthyОценок пока нет
- Maternity Hospital Near MeДокумент7 страницMaternity Hospital Near MeFemiint HealthОценок пока нет
- Greenwich Hospital MapДокумент1 страницаGreenwich Hospital Mapomegasauron0gmailcomОценок пока нет
- Clinical Handover Ian ScottДокумент26 страницClinical Handover Ian ScottYwagar YwagarОценок пока нет
- Perioperative Care of The Child: A Nursing Manual: October 2010 Vol 92 No4Документ2 страницыPerioperative Care of The Child: A Nursing Manual: October 2010 Vol 92 No4Pahang Reforansa PutraОценок пока нет
- September 21, 2018 Strathmore TimesДокумент24 страницыSeptember 21, 2018 Strathmore TimesStrathmore TimesОценок пока нет
- Klasifikasi AramanyДокумент7 страницKlasifikasi AramanyErwin SutonoОценок пока нет
- Osei Afriyie Samuel's Industrial Attachment ReportДокумент20 страницOsei Afriyie Samuel's Industrial Attachment Reportoseiafriyiesamuel80% (5)
- Comparision Between Provisional Diagnosis Made in Emergency Department VS Final Discharge Diagnosis at Ramkrishna Care Hospital, Raipur C.GДокумент14 страницComparision Between Provisional Diagnosis Made in Emergency Department VS Final Discharge Diagnosis at Ramkrishna Care Hospital, Raipur C.GIJAR JOURNALОценок пока нет
- Biovac DrainДокумент6 страницBiovac Drainjames100% (1)
- LAPORAN KEGIATAN RESIDENSI HARI KE 2 Di RS SIRIRAJДокумент24 страницыLAPORAN KEGIATAN RESIDENSI HARI KE 2 Di RS SIRIRAJIhrom Fatma SaputriОценок пока нет
- Transactional An. 002 062-02Документ12 страницTransactional An. 002 062-02Richard DodsonОценок пока нет
- Review of Related Literature 2.1 Related Literature 2.1.1 Foreign ResearchesДокумент42 страницыReview of Related Literature 2.1 Related Literature 2.1.1 Foreign ResearchesAt Sa Wakas AyОценок пока нет
- Discharge SummaryДокумент2 страницыDischarge SummaryJaslynn WhiteОценок пока нет
- Huron Hometown News - October 24, 2013Документ10 страницHuron Hometown News - October 24, 2013Catawba SecurityОценок пока нет
- Resuscitation: Richard A. Field, Zoë Fritz, Annalie Baker, Amy Grove, Gavin D. PerkinsДокумент14 страницResuscitation: Richard A. Field, Zoë Fritz, Annalie Baker, Amy Grove, Gavin D. PerkinsFira GorjessОценок пока нет
- New Document Mcqs EpidemiologyДокумент51 страницаNew Document Mcqs EpidemiologySurgeonZak100% (1)
- Hi Alert MedicationsHHHIGHДокумент27 страницHi Alert MedicationsHHHIGHnovitalumintusariОценок пока нет
- SBR - RPN ResumeДокумент3 страницыSBR - RPN Resumeapi-283976731Оценок пока нет
- 63 - CASE REPORT Epulis GranulomaДокумент3 страницы63 - CASE REPORT Epulis GranulomaRina NovitrianiОценок пока нет
- The Book of The Rotunda HospitalДокумент342 страницыThe Book of The Rotunda HospitalGeordie WinkleОценок пока нет
- In-Service Training Programs For Nurses, 1st and 2nd Quarter, Calendar Year 2023Документ4 страницыIn-Service Training Programs For Nurses, 1st and 2nd Quarter, Calendar Year 2023iamxai rnmanemtОценок пока нет
- TS Workbook 3Документ150 страницTS Workbook 3Sara da Silva100% (1)
- PAPO Statement Regarding The PhilHealth Cataract Operations ScandalДокумент5 страницPAPO Statement Regarding The PhilHealth Cataract Operations ScandalJess LorenzoОценок пока нет
- MDC EHS Progress Report Presentation 21 Nov 09Документ37 страницMDC EHS Progress Report Presentation 21 Nov 09Eze FoncardasОценок пока нет
- Ozgundondu 2019Документ10 страницOzgundondu 2019ARINAОценок пока нет
- R. D. Laing: Contemporary Perspectives: References ReprintsДокумент7 страницR. D. Laing: Contemporary Perspectives: References ReprintsashfaqamarОценок пока нет
- MEP Planning GuideДокумент67 страницMEP Planning GuideIshan Ranganath100% (1)
- Role of PharmacistДокумент9 страницRole of PharmacistAbid Ali Khan0% (1)