Вам также может понравиться
- Essay 2011Документ2 страницыEssay 2011zakhanisbОценок пока нет
- Applied Maths SubjectiveДокумент2 страницыApplied Maths SubjectiveMuhammad Talha MunirОценок пока нет
- Caf05 ST 2017Документ288 страницCaf05 ST 2017usmanОценок пока нет
- Caf05 ST 2017Документ288 страницCaf05 ST 2017usmanОценок пока нет
- Indian OceanДокумент3 страницыIndian OceanusmanОценок пока нет
- OBOR Project of Century: The Asian FortressДокумент20 страницOBOR Project of Century: The Asian FortressusmanОценок пока нет
- Diseases of The PleuraДокумент35 страницDiseases of The PleurausmanОценок пока нет
- Foot and Ankle 2013 HOДокумент7 страницFoot and Ankle 2013 HOusmanОценок пока нет
- T & L Spine 2013 HOДокумент4 страницыT & L Spine 2013 HOusmanОценок пока нет
- Chest TraumaДокумент77 страницChest TraumausmanОценок пока нет
- A A AДокумент401 страницаA A ADaniel Eguakun100% (1)
- General Principles Spine 2013 HOДокумент4 страницыGeneral Principles Spine 2013 HOusmanОценок пока нет
- Pelvis 2013 HOДокумент10 страницPelvis 2013 HOusmanОценок пока нет
- EthicsДокумент7 страницEthicsusmanОценок пока нет
- Cardiovascular Disease 2014 HOДокумент8 страницCardiovascular Disease 2014 HOusmanОценок пока нет
- Healthcare ProfessionalДокумент26 страницHealthcare ProfessionalusmanОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Product Catalogue 2010Документ112 страницProduct Catalogue 2010Dennis NguyenОценок пока нет
- Military Working Dog ProgramДокумент155 страницMilitary Working Dog Programjojo2486100% (3)
- Together With YouДокумент39 страницTogether With YouBethany House Publishers100% (1)
- Practice Subject and Verb IdentificationДокумент4 страницыPractice Subject and Verb IdentificationAyuseptiОценок пока нет
- Un SMP 2016Документ27 страницUn SMP 2016SmpMugaruОценок пока нет
- Chapter 7 Study GuideДокумент4 страницыChapter 7 Study GuidejbradeeОценок пока нет
- Assessment of NewbornДокумент26 страницAssessment of Newbornaybee_14Оценок пока нет
- Pulpal Reactions To Caries and Dental ProceduresДокумент58 страницPulpal Reactions To Caries and Dental ProceduresSony RajbhandariОценок пока нет
- Syphilis, or The French DiseaseДокумент5 страницSyphilis, or The French DiseaseLiz SernaОценок пока нет
- Deteksi Seksual Dimorfisme Pada Benih Ikan Tawes (Barbomymus Gonionotus Bleeker, 1850) Berdasarkan Morfologi Dan AnatomiДокумент13 страницDeteksi Seksual Dimorfisme Pada Benih Ikan Tawes (Barbomymus Gonionotus Bleeker, 1850) Berdasarkan Morfologi Dan AnatomiSiwiana Dinar UtaminingtyasОценок пока нет
- World's Most Awesome Invertebrate: Activity Subject: Invertebrate Biodiversity Grade Level: 7 - 12 GradesДокумент5 страницWorld's Most Awesome Invertebrate: Activity Subject: Invertebrate Biodiversity Grade Level: 7 - 12 GradesVeraОценок пока нет
- Img 3212Документ2 страницыImg 3212Douglas JoynerОценок пока нет
- Inbo 2009Документ42 страницыInbo 2009BenjaminVasileniucОценок пока нет
- Latihan Soal Bahasa Inggris Sma Kelas X Semester 2Документ14 страницLatihan Soal Bahasa Inggris Sma Kelas X Semester 2tyasajeng100% (2)
- DR Mushtaq Amna Ashraf Aqsa Bashir Ayesha Bibi Hira Nisar Iqra HabibДокумент5 страницDR Mushtaq Amna Ashraf Aqsa Bashir Ayesha Bibi Hira Nisar Iqra HabibtaibiОценок пока нет
- CLS Aipmt-19-20 XI Zoo Study-Package-1 Level-1 Chapter-1 PDFДокумент20 страницCLS Aipmt-19-20 XI Zoo Study-Package-1 Level-1 Chapter-1 PDFJainil PatelОценок пока нет
- List of SlaughterHouses in UAEДокумент2 страницыList of SlaughterHouses in UAEDr-Muhammad Awais Ch100% (1)
- Laxative and Purgative HerbsДокумент2 страницыLaxative and Purgative HerbsqueencelОценок пока нет
- Autobiography V BiographyДокумент22 страницыAutobiography V BiographyRuchiKhannaОценок пока нет
- The Integumentary System: Powerpoint Lecture Slides Prepared by Meg Flemming Austin Community CollegeДокумент62 страницыThe Integumentary System: Powerpoint Lecture Slides Prepared by Meg Flemming Austin Community CollegetanarОценок пока нет
- Harcourt GK Phonics Practice Book StudentДокумент144 страницыHarcourt GK Phonics Practice Book StudentІрина КрупаОценок пока нет
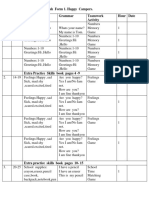
- English Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour DateДокумент4 страницыEnglish Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour Dateİlkanə CabbarovaОценок пока нет
- Dairyrobot r9500 Automated Robotic Milking 253951Документ15 страницDairyrobot r9500 Automated Robotic Milking 253951Sahil ShahОценок пока нет
- Beliefs and SuperstitionsДокумент1 страницаBeliefs and Superstitionsmcharrel90Оценок пока нет
- Mind and Memory TrainingДокумент268 страницMind and Memory Trainingysbrar200850% (2)
- ?weebee Beginners Bunny CALДокумент17 страниц?weebee Beginners Bunny CALyovanna ortizОценок пока нет
- Creatures & Constructs A Monster Manual Supplement For EberronДокумент74 страницыCreatures & Constructs A Monster Manual Supplement For EberronJason BryantОценок пока нет
- Animal WordsДокумент2 страницыAnimal WordsSandra GarcíaОценок пока нет
- Basic Anatomy and Physiology of Brain and Spinal CordДокумент59 страницBasic Anatomy and Physiology of Brain and Spinal CorddrmalikarifОценок пока нет
- FOM STUDY GUIDE 3rd Block 1Документ3 страницыFOM STUDY GUIDE 3rd Block 1Bernadine Cruz Par100% (1)