Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- .A Gift From The Stars PDFДокумент186 страниц.A Gift From The Stars PDFAivlys100% (1)
- In Re Sars-Cov-2 Verified Complaint Jury Trial DemandedДокумент64 страницыIn Re Sars-Cov-2 Verified Complaint Jury Trial DemandedSarah Westall100% (2)
- Anchor Design ManualДокумент388 страницAnchor Design ManualJianhua WuОценок пока нет
- Bacillinum-Experiences and StudyДокумент7 страницBacillinum-Experiences and Studyssrkm guptaОценок пока нет
- Ebook PDF An Invitation To Health Taking Charge of Your Health 19th EditionДокумент61 страницаEbook PDF An Invitation To Health Taking Charge of Your Health 19th Editionjohn.ward557100% (44)
- Grade 9 12 SMAWДокумент10 страницGrade 9 12 SMAWFlor Gagasa100% (4)
- Writing An Abstract For Your Research Paper PDFДокумент9 страницWriting An Abstract For Your Research Paper PDFabcbatata0% (1)
- Evolve 5 - Mid Term Test ReviewДокумент9 страницEvolve 5 - Mid Term Test ReviewLaiza Godoy100% (3)
- Principles of Landscape & Regional EcologyДокумент10 страницPrinciples of Landscape & Regional EcologyJúnior SenseyОценок пока нет
- Stoeckle Thaler Final Reduced 002Документ30 страницStoeckle Thaler Final Reduced 002Júnior SenseyОценок пока нет
- Land-Use Changes in SouthernДокумент20 страницLand-Use Changes in SouthernJúnior SenseyОценок пока нет
- Diversity of Cyperaceae in BrazilДокумент12 страницDiversity of Cyperaceae in BrazilJúnior SenseyОценок пока нет
- A Synopsis of The Rubiaceae of The States of Mato Grosso and Mato Grosso Do Sul, Brazil, With A Key To Genera, and A Preliminary Species ListДокумент84 страницыA Synopsis of The Rubiaceae of The States of Mato Grosso and Mato Grosso Do Sul, Brazil, With A Key To Genera, and A Preliminary Species ListJúnior SenseyОценок пока нет
- Nomenclatural Notes On Varronia (Boraginaceae) in BrazilДокумент3 страницыNomenclatural Notes On Varronia (Boraginaceae) in BrazilJúnior SenseyОценок пока нет
- A Note On Contagion Indices For Landscape AnalysisДокумент6 страницA Note On Contagion Indices For Landscape AnalysisJúnior SenseyОценок пока нет
- 10.1007 BF00137155Документ23 страницы10.1007 BF00137155Júnior SenseyОценок пока нет
- Distance From Roads and Cities As A Predictor of Habitat Loss and Fragmentation in The Caatinga Vegetation of Brazil Santos & Tabarelli 2002Документ9 страницDistance From Roads and Cities As A Predictor of Habitat Loss and Fragmentation in The Caatinga Vegetation of Brazil Santos & Tabarelli 2002Júnior SenseyОценок пока нет
- Active and Passive Euthanasia Thesis StatementДокумент7 страницActive and Passive Euthanasia Thesis StatementDoMyPaperForMeSingapore100% (2)
- Trauma Case Reports: Jugert Bango, Evan Zhang, Daniel L. Aaron, Amna DiwanДокумент4 страницыTrauma Case Reports: Jugert Bango, Evan Zhang, Daniel L. Aaron, Amna DiwanCristhian Jover CastroОценок пока нет
- 英文閱讀理解|Reading - hikikomoriДокумент11 страниц英文閱讀理解|Reading - hikikomoriArLokОценок пока нет
- Simple ModelsДокумент52 страницыSimple ModelsRohan sharmaОценок пока нет
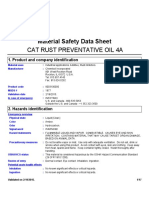
- 4a Rust Preventive OilДокумент17 страниц4a Rust Preventive OilBalaji DDОценок пока нет
- Nderstanding Normal and Clinical Nutrition 9th Edition Rolfes Test BankДокумент35 страницNderstanding Normal and Clinical Nutrition 9th Edition Rolfes Test Bankescout.stoopvr5nbf100% (24)
- List of The State Govt. Employees To Retire On 31.01.2020: Series A/C - No Subscr - Name DOB DOR TRY DesgДокумент24 страницыList of The State Govt. Employees To Retire On 31.01.2020: Series A/C - No Subscr - Name DOB DOR TRY DesgManish GuptaОценок пока нет
- Types and Procedures of DialysisДокумент8 страницTypes and Procedures of DialysisKristine PangahinОценок пока нет
- 6 CBLM - UC1 Carry Out Minor Vehicle MaintenanceДокумент127 страниц6 CBLM - UC1 Carry Out Minor Vehicle MaintenanceTESDA Lazi Technical InstituteОценок пока нет
- GAD7Документ2 страницыGAD7Alice Bonnie CaulfieldОценок пока нет
- Brad Hinton CVДокумент6 страницBrad Hinton CVapi-486072801Оценок пока нет
- Drugs )Документ2 страницыDrugs )Brandon Lingo LeeОценок пока нет
- Guidelines Adult Advanced Life SupportДокумент34 страницыGuidelines Adult Advanced Life SupportParvathy R NairОценок пока нет
- Health Effects of Sleep DeprivationДокумент7 страницHealth Effects of Sleep DeprivationEmily KajlaОценок пока нет
- Name: Muhammad Jazim Reg # L1F20BSCE0024 Subject: English - II Depression in The TeenageДокумент2 страницыName: Muhammad Jazim Reg # L1F20BSCE0024 Subject: English - II Depression in The TeenageM jazimОценок пока нет
- Direction: Choose The Correct Answer To Complete The Sentences!Документ7 страницDirection: Choose The Correct Answer To Complete The Sentences!M hilmi hidayatullahОценок пока нет
- Apgvb Insurance Consent LetterДокумент1 страницаApgvb Insurance Consent LetterMahesh PasupuletiОценок пока нет
- Affidavit Age ChangeДокумент206 страницAffidavit Age ChangeMir ImranОценок пока нет
- Junal ScreeningДокумент9 страницJunal ScreeningRama BayuОценок пока нет
- m6 Endocrine System - Lesson 1 HormonesДокумент32 страницыm6 Endocrine System - Lesson 1 HormonesJunimar AggabaoОценок пока нет
- New Microsoft Word DocumentДокумент2 страницыNew Microsoft Word DocumentMaureenОценок пока нет
- GAP CERTIFICATE AFFIDAVITДокумент2 страницыGAP CERTIFICATE AFFIDAVITRAJESHREE MAHANGADEОценок пока нет