Вам также может понравиться
- Cross-Training: The Medical Assistant WorkbookОт EverandCross-Training: The Medical Assistant WorkbookОценок пока нет
- Employment Practices Liability: Guide to Risk Exposures and Coverage, 2nd EditionОт EverandEmployment Practices Liability: Guide to Risk Exposures and Coverage, 2nd EditionОценок пока нет
- UNUM Brochure 1.1.2020Документ4 страницыUNUM Brochure 1.1.2020icbinwОценок пока нет
- USDOS ASPE Health Plan Contact and Claims InfoДокумент1 страницаUSDOS ASPE Health Plan Contact and Claims InfoEstrella Cotrina RojasОценок пока нет
- The NoticeДокумент5 страницThe NoticeMayra ParrillaОценок пока нет
- First Aid Record Form: InstructionsДокумент4 страницыFirst Aid Record Form: InstructionsExperienceCentre vjnrОценок пока нет
- Formatos Axa ExtranjerosДокумент2 страницыFormatos Axa ExtranjerosLev AnahОценок пока нет
- First Aid Record Form KitДокумент4 страницыFirst Aid Record Form KitExperienceCentre vjnrОценок пока нет
- Asurion Documentation Process: RequiredДокумент2 страницыAsurion Documentation Process: RequiredDave GonzalesОценок пока нет
- Ofs Era Claim FormДокумент2 страницыOfs Era Claim Formbanira.luv3000Оценок пока нет
- Main Notice of Injury or Occupational Disease Incident Report NevadaДокумент2 страницыMain Notice of Injury or Occupational Disease Incident Report NevadaSamier MohamedОценок пока нет
- 2048 - Wal - DL - STD Initial Packet - APS PKT PDFДокумент21 страница2048 - Wal - DL - STD Initial Packet - APS PKT PDFWalter AguilarОценок пока нет
- Asurion Claim Affidavit PDFДокумент2 страницыAsurion Claim Affidavit PDFJoseph Reid60% (5)
- MetLife Basic GTL CertificateДокумент63 страницыMetLife Basic GTL Certificatereddyraj036Оценок пока нет
- Claimant Rights and Responsibilities Rules For Filing A Claim and Appeal RightsДокумент7 страницClaimant Rights and Responsibilities Rules For Filing A Claim and Appeal Rightsanon_26882226Оценок пока нет
- Medical Billing Process: Naveen MajetyДокумент21 страницаMedical Billing Process: Naveen MajetyNaveen KumarОценок пока нет
- 5 Min InjuryorIllness 3Документ3 страницы5 Min InjuryorIllness 3ikperha jomafuvweОценок пока нет
- Oman New Reimbursement Claim FormДокумент3 страницыOman New Reimbursement Claim Formtoalok4723Оценок пока нет
- Virginia D. Long: 4224 W. Charleston # 171 Las Vegas NV 89102Документ3 страницыVirginia D. Long: 4224 W. Charleston # 171 Las Vegas NV 89102Abrar_AshrafОценок пока нет
- FlexIT OPD Domiciliary ClaimДокумент4 страницыFlexIT OPD Domiciliary ClaimColorful ChilakaОценок пока нет
- Claim FormДокумент4 страницыClaim Formmuhammad haroonОценок пока нет
- Claim Form Dd2642Документ4 страницыClaim Form Dd2642Adina BusteaОценок пока нет
- Understanding The Consumer Complaint ProcessДокумент2 страницыUnderstanding The Consumer Complaint ProcessTitle IV-D Man with a planОценок пока нет
- Best Practices For Complex Liability ClaimsДокумент62 страницыBest Practices For Complex Liability ClaimsAPAResultsОценок пока нет
- Asurion Claim DocsДокумент2 страницыAsurion Claim DocsCr JaxОценок пока нет
- Health Care Provider ReportДокумент2 страницыHealth Care Provider ReportsiskjereОценок пока нет
- 14 BOSH - Module 6 Employees Compensation ProgramДокумент29 страниц14 BOSH - Module 6 Employees Compensation Programbeng acostaОценок пока нет
- Asurion Documentation Process StepsДокумент2 страницыAsurion Documentation Process StepsReap PadenОценок пока нет
- Assurant Health Access: in Force Underwriting Change PacketДокумент10 страницAssurant Health Access: in Force Underwriting Change PacketSwisskelly1Оценок пока нет
- Professional Responsibility Concern Fillable FormДокумент1 страницаProfessional Responsibility Concern Fillable FormWendy YОценок пока нет
- Physician. Submittal of A Completed DWC-1 ClaimДокумент2 страницыPhysician. Submittal of A Completed DWC-1 ClaimXYZОценок пока нет
- Important Information2Документ5 страницImportant Information2api-416112264Оценок пока нет
- 3 Consumer Safety SolutionsДокумент3 страницы3 Consumer Safety Solutionstimeless wunОценок пока нет
- Continuing Disability Claim Form English 10-19-22Документ4 страницыContinuing Disability Claim Form English 10-19-22Michelle LeeОценок пока нет
- Industrial Commission of Arizona: Workers' Compensation Information For The Injured WorkerДокумент12 страницIndustrial Commission of Arizona: Workers' Compensation Information For The Injured WorkerdejewsonОценок пока нет
- Asurion AffidavitДокумент2 страницыAsurion AffidavitErnestRobinson100% (1)
- Claim Process PDFДокумент2 страницыClaim Process PDFpizza nmorevikОценок пока нет
- Medicaid AppealДокумент15 страницMedicaid Appealmtp7389Оценок пока нет
- AXA Non Death Claim FormДокумент4 страницыAXA Non Death Claim FormKenji ChinОценок пока нет
- Policy-401-Accident-Procedures-Dec-2008 2Документ4 страницыPolicy-401-Accident-Procedures-Dec-2008 2syamimi balkhisОценок пока нет
- How To Appeal A FEMA Disaster Assistance DecisionДокумент2 страницыHow To Appeal A FEMA Disaster Assistance DecisionKristi ParfaitОценок пока нет
- What To Do Following A Workplace AccidentДокумент5 страницWhat To Do Following A Workplace AccidentMona DeldarОценок пока нет
- Claims HandbookДокумент6 страницClaims Handbookvivekca.webloginОценок пока нет
- Of India: 'L:FTMДокумент14 страницOf India: 'L:FTMPrudhvi ReddyОценок пока нет
- Doctor Statement Ssa 787Документ3 страницыDoctor Statement Ssa 787Richard GuthОценок пока нет
- Protecting Your Business and Employees From Identity TheftДокумент2 страницыProtecting Your Business and Employees From Identity TheftClickon DetroitОценок пока нет
- How To Appeal A Health Care Insurance Decision - OIC 2019Документ62 страницыHow To Appeal A Health Care Insurance Decision - OIC 2019Jeff ReifmanОценок пока нет
- OSHA Form 300 and 301 RecordsДокумент6 страницOSHA Form 300 and 301 Recordsiese027Оценок пока нет
- Back To WorkДокумент24 страницыBack To WorklanchuОценок пока нет
- FAA MedXPress Program For PilotsДокумент6 страницFAA MedXPress Program For PilotsIctor PrinceОценок пока нет
- Unity Point Phishing ScamДокумент1 страницаUnity Point Phishing ScamdmronlineОценок пока нет
- Tips For Making A Successful Work Accident Claim de La Garza Law FirmДокумент4 страницыTips For Making A Successful Work Accident Claim de La Garza Law FirmcokecarrilloОценок пока нет
- Faq PDFДокумент3 страницыFaq PDFnadine hermocillaОценок пока нет
- l Hi Appt Documents 02272023Документ9 страницl Hi Appt Documents 02272023gelosmith3Оценок пока нет
- Consumers TakeactionДокумент22 страницыConsumers TakeactionMai WholenameОценок пока нет
- Ap 101Документ2 страницыAp 101Anita KosticОценок пока нет
- Claim Facilitation Form 2019 - RTMДокумент2 страницыClaim Facilitation Form 2019 - RTMDick Cheney100% (1)
- OSHA Citation of Fairview Contractors Inc. of Lee, Ma.Документ15 страницOSHA Citation of Fairview Contractors Inc. of Lee, Ma.Patrick JohnsonОценок пока нет
- OVHC Claim Form 102017 PDFДокумент3 страницыOVHC Claim Form 102017 PDFtarmudiОценок пока нет
- f10 Claim FormДокумент2 страницыf10 Claim Formiceslurpie100% (1)
- The Economic Times April 262020Документ22 страницыThe Economic Times April 262020Diana MОценок пока нет
- Resource For Question 2 - Parts (A) and (B)Документ2 страницыResource For Question 2 - Parts (A) and (B)Aung Zaw HtweОценок пока нет
- Geith Contact List 03-2014Документ3 страницыGeith Contact List 03-2014jrincon26Оценок пока нет
- 3 Rs of Waste Management - Reduce, Reuse, RecycleДокумент2 страницы3 Rs of Waste Management - Reduce, Reuse, RecycleCOSGA CaloocanОценок пока нет
- Achieving Customer Service ExcellenceДокумент16 страницAchieving Customer Service ExcellenceRoy CabarlesОценок пока нет
- Accruals Accounting: A Brief Guide ToДокумент4 страницыAccruals Accounting: A Brief Guide Tosrihari44188Оценок пока нет
- ICC non-circumvention agreementДокумент14 страницICC non-circumvention agreementZR IKОценок пока нет
- Activist Spotlight - Abhilasha - A - SinghДокумент14 страницActivist Spotlight - Abhilasha - A - SinghSikh Parent LeaderОценок пока нет
- FCM Services FeaturesДокумент86 страницFCM Services FeaturesTing ohn100% (1)
- VYVO Business Presentation ENGДокумент54 страницыVYVO Business Presentation ENGԱբրենիկա ՖերլինОценок пока нет
- Domain GraduateДокумент77 страницDomain GraduateNecessity BDОценок пока нет
- Safe Use Lorry Cranes LoaderДокумент23 страницыSafe Use Lorry Cranes LoaderBigbearBigbearОценок пока нет
- 2012 The Darwinian Workplace.Документ4 страницы2012 The Darwinian Workplace.kasireddyvarun98Оценок пока нет
- LP Sample Model Formulation, Duality, Sensitivity Analysis Product MixДокумент8 страницLP Sample Model Formulation, Duality, Sensitivity Analysis Product MixZed Alemayehu100% (1)
- Problems On Cash Budget MBAДокумент3 страницыProblems On Cash Budget MBAsafwanhossain100% (1)
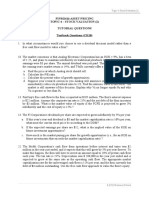
- Tutorial 4 QuestionsДокумент4 страницыTutorial 4 Questionsguan junyan0% (1)
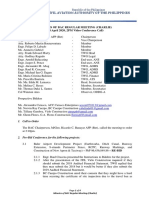
- Minutes BAC Charlie April 14 2020Документ4 страницыMinutes BAC Charlie April 14 2020Desiree AllonesОценок пока нет
- The Management Process: Learning OutcomesДокумент37 страницThe Management Process: Learning OutcomesTumisang MAVUSOОценок пока нет
- Bank Confirmation FormatДокумент4 страницыBank Confirmation FormatTasdik MahmudОценок пока нет
- فرانسيس اكسفير - فينجتون-Rent Agmt. - FingtonДокумент8 страницفرانسيس اكسفير - فينجتون-Rent Agmt. - FingtonChristina FingtonОценок пока нет
- Indian Startup Ecosystem Journey Post-COVIDДокумент17 страницIndian Startup Ecosystem Journey Post-COVIDKetaki OgaleОценок пока нет
- Unit 1 Introduction Journal Ledger and Trial BalanceДокумент51 страницаUnit 1 Introduction Journal Ledger and Trial Balancedivimba87100% (1)
- Assignment 1Документ2 страницыAssignment 1Eden teklemariamОценок пока нет
- Hajar TAQI: Education Work ExperiencesДокумент1 страницаHajar TAQI: Education Work ExperiencesMozammel AhmedОценок пока нет
- Financial management paper investment decisionsДокумент28 страницFinancial management paper investment decisions2154 taibakhatunОценок пока нет
- MBA Syllabus Guide for Organizational Change and DevelopmentДокумент144 страницыMBA Syllabus Guide for Organizational Change and Developmentprasadkh90Оценок пока нет
- Example 2 PresentationДокумент53 страницыExample 2 Presentationrivandi farren tanayaОценок пока нет
- Monitor Flare Stacks and Reduce Pollution with IR CamerasДокумент4 страницыMonitor Flare Stacks and Reduce Pollution with IR CamerasayviwurbayviwurbОценок пока нет
- Unique Punch Systems Pvt. LTD.: QuotationДокумент2 страницыUnique Punch Systems Pvt. LTD.: QuotationMechanical DesignОценок пока нет
- A Case Study Analysis of Factors For Success in ERP System ImplementationsДокумент8 страницA Case Study Analysis of Factors For Success in ERP System Implementationsأميرة جمالОценок пока нет