Вам также может понравиться
- Steel Casting HandbookДокумент74 страницыSteel Casting Handbooktang weng wai100% (2)
- Region Iv-A Calabarzon Department of Education Bitin Integrated National High SchoolДокумент4 страницыRegion Iv-A Calabarzon Department of Education Bitin Integrated National High SchoolAlbert Ian Casuga100% (1)
- Zoonotic DiseaseДокумент34 страницыZoonotic Diseasebajarangi_chaudhary100% (2)
- HandBook Stuctural SteelДокумент267 страницHandBook Stuctural SteelOnn Lajer100% (9)
- HandBook Stuctural SteelДокумент267 страницHandBook Stuctural SteelOnn Lajer100% (9)
- HandBook Stuctural SteelДокумент267 страницHandBook Stuctural SteelOnn Lajer100% (9)
- Ultrasonic Testing of Steel CastingДокумент38 страницUltrasonic Testing of Steel CastingPARK, SANGYEOLОценок пока нет
- Ultrasonic Testing of Steel CastingДокумент38 страницUltrasonic Testing of Steel CastingPARK, SANGYEOLОценок пока нет
- Bacteriophages in Health and DiseaseДокумент297 страницBacteriophages in Health and DiseaseCisticola100% (1)
- Process SafetyДокумент15 страницProcess SafetyWormInchОценок пока нет
- S5-Steel Casting HandbookДокумент26 страницS5-Steel Casting HandbookCharlie ChongОценок пока нет
- S5-Steel Casting HandbookДокумент26 страницS5-Steel Casting HandbookCharlie ChongОценок пока нет
- S5-Steel Casting HandbookДокумент26 страницS5-Steel Casting HandbookCharlie ChongОценок пока нет
- DEATH STATISTICS - IFR 0,01% - A Tribute To The Corona Virus Whistle Blowers - TRANSLATION MANY LANGUAGES ATДокумент47 страницDEATH STATISTICS - IFR 0,01% - A Tribute To The Corona Virus Whistle Blowers - TRANSLATION MANY LANGUAGES ATPeter100% (2)
- What Is Rabies?Документ9 страницWhat Is Rabies?Bijay Kumar MahatoОценок пока нет
- Zoonotic Diseases 1Документ2 страницыZoonotic Diseases 1MelОценок пока нет
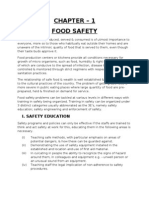
- Chapter - 1 Food SafetyДокумент30 страницChapter - 1 Food Safetychefjaved82% (28)
- Best Practices in Infection Prevention and Control PDFДокумент198 страницBest Practices in Infection Prevention and Control PDFYunita Panjaitan100% (2)
- ChikungunyaДокумент61 страницаChikungunyaE. B. F.Оценок пока нет
- Monkey PoxДокумент4 страницыMonkey PoxPrince Mark BadilloОценок пока нет
- (Welding) s7Документ113 страниц(Welding) s7Popo YuppyОценок пока нет
- (Welding) s7Документ113 страниц(Welding) s7Popo YuppyОценок пока нет
- The Infection Game Supplement: new infections, retroviruses and pandemicsОт EverandThe Infection Game Supplement: new infections, retroviruses and pandemicsОценок пока нет
- 3.01.05 CCHFДокумент8 страниц3.01.05 CCHFkcstincasОценок пока нет
- 3.01.05 CCHFДокумент9 страниц3.01.05 CCHFEl GhazaliОценок пока нет
- Communicable Diseases Surveillance and Response CCHF Fact Sheet SEAROДокумент4 страницыCommunicable Diseases Surveillance and Response CCHF Fact Sheet SEAROLakshmi SethОценок пока нет
- Human MonkeypoxДокумент17 страницHuman MonkeypoxJessica C. S.Оценок пока нет
- CCHFДокумент12 страницCCHFmitaОценок пока нет
- Microorganisms 11 01138Документ14 страницMicroorganisms 11 01138pramitpatelphotographyОценок пока нет
- REVIEWA Naplasma Marginale and Anaplasma Phagocytophilum-Rickettsiales Pathogens of Veterinary and Publichealth SignificanceДокумент17 страницREVIEWA Naplasma Marginale and Anaplasma Phagocytophilum-Rickettsiales Pathogens of Veterinary and Publichealth Significanceyudhi arjentiniaОценок пока нет
- Transmission Dynamics of Crimean-Congo HaemorrhagiДокумент17 страницTransmission Dynamics of Crimean-Congo Haemorrhagiali zohaibОценок пока нет
- Main 2Документ18 страницMain 2YTP MạnhОценок пока нет
- Crimean-Congo Hemorrhagic Fever: TransmissionДокумент2 страницыCrimean-Congo Hemorrhagic Fever: TransmissionMoin DilawarОценок пока нет
- Humanmonkeypox: Epidemiologic and Clinical Characteristics, Diagnosis, and PreventionДокумент17 страницHumanmonkeypox: Epidemiologic and Clinical Characteristics, Diagnosis, and PreventionAlejandro GraterolОценок пока нет
- Ebola Virus Disease: Key FactsДокумент3 страницыEbola Virus Disease: Key FactsruguОценок пока нет
- Shiva Chandra 2011Документ16 страницShiva Chandra 2011Spica RegulusОценок пока нет
- Swine Influenza: Nature of The DiseaseДокумент8 страницSwine Influenza: Nature of The Diseasejawairia_mmgОценок пока нет
- Crimean Congo Hemorrhagic FeverДокумент18 страницCrimean Congo Hemorrhagic FeverAmmar AbbasОценок пока нет
- Epidemiology of Avian Influenza in GhanaДокумент5 страницEpidemiology of Avian Influenza in GhanaYvonne Sorviel SiiloОценок пока нет
- Solignat Et Al. - 2009 - Replication Cycle of Chikungunya A Re-Emerging ArbovirusДокумент15 страницSolignat Et Al. - 2009 - Replication Cycle of Chikungunya A Re-Emerging ArbovirusLaise Eduarda Paixão de MoraesОценок пока нет
- Ticks On The Run: A Mathematical Model of Crimean-Congo Haemorrhagic Fever (CCHF) - Key Factors For TransmissionДокумент47 страницTicks On The Run: A Mathematical Model of Crimean-Congo Haemorrhagic Fever (CCHF) - Key Factors For TransmissionChristopher ServantОценок пока нет
- PRRS Guide Web Bulletin - OIEДокумент7 страницPRRS Guide Web Bulletin - OIESimone Rosa DidonéОценок пока нет
- African Swine FeverДокумент5 страницAfrican Swine FeverPhilein YlaganОценок пока нет
- Rabies Vaccines WHO Position PaperДокумент14 страницRabies Vaccines WHO Position PaperMark Anthony BernasОценок пока нет
- Topic: "Picoronoviruses. Coxsackie. ECHO. Laboratory Diagnostics"Документ26 страницTopic: "Picoronoviruses. Coxsackie. ECHO. Laboratory Diagnostics"deekshit dcОценок пока нет
- Petersen Human Monkeypox Rev ID Clin NA 2019Документ17 страницPetersen Human Monkeypox Rev ID Clin NA 2019thaistoledofinkОценок пока нет
- Pathogenesis of Ruminant Herpesvirus Infections: Monika Engels, Mathias AckermannДокумент13 страницPathogenesis of Ruminant Herpesvirus Infections: Monika Engels, Mathias AckermannRosafina SetyantariОценок пока нет
- Salmonellosisincluding Entericfever: Farah Naz Qamar,, Wajid Hussain,, Sonia QureshiДокумент13 страницSalmonellosisincluding Entericfever: Farah Naz Qamar,, Wajid Hussain,, Sonia QureshiAnak MuadzОценок пока нет
- Arboviruses in ChinaДокумент21 страницаArboviruses in ChinaChris LicínioОценок пока нет
- Ebola Virus - Pathogen Safety Data SheetsДокумент7 страницEbola Virus - Pathogen Safety Data SheetsLela Wahyu AnggraeniОценок пока нет
- WHO - Ebola Virus Disease (Evd) Key FactsДокумент6 страницWHO - Ebola Virus Disease (Evd) Key FactsBeatrice IoanaОценок пока нет
- West Nile Fever: C H A P T E R 2 - 1 - 2 0Документ12 страницWest Nile Fever: C H A P T E R 2 - 1 - 2 0WormInchОценок пока нет
- 1 See The Note in Chapter 2.9.8 Salmonellosis For The Principles Followed Concerning The Nomenclature of SalmonellaДокумент17 страниц1 See The Note in Chapter 2.9.8 Salmonellosis For The Principles Followed Concerning The Nomenclature of SalmonellaWira RamayadiОценок пока нет
- Ebola Virus DiseaseДокумент13 страницEbola Virus DiseaseMade Sudarsana0% (1)
- Ni Hms 902603Документ44 страницыNi Hms 902603saminurichard2017Оценок пока нет
- Ebola Virus Disease (WHO) : Key FactsДокумент5 страницEbola Virus Disease (WHO) : Key FactsridhosetyawanОценок пока нет
- Human Monkeypox Epidemiologic and Clinical Characteristics, Diagnosis, and PreventionДокумент17 страницHuman Monkeypox Epidemiologic and Clinical Characteristics, Diagnosis, and PreventionVeronicaSanJoséОценок пока нет
- Bird FluДокумент21 страницаBird FluARG ShovonОценок пока нет
- Clin Gui EncephalitisДокумент9 страницClin Gui EncephalitisAl MuzakkiОценок пока нет
- Avian Influenza A (H5N1) : A Preliminary ReviewДокумент4 страницыAvian Influenza A (H5N1) : A Preliminary ReviewvijayОценок пока нет
- AvianPneumovirus APV PDFДокумент7 страницAvianPneumovirus APV PDFRayza Lubis0% (1)
- What's Monkeypox ?Документ10 страницWhat's Monkeypox ?Fumika VenayaОценок пока нет
- Review On Epidemiology and Pathology of Yellow Fever VirusДокумент24 страницыReview On Epidemiology and Pathology of Yellow Fever Virushenok bushura100% (1)
- Detection of Newcastle Disease Virus in PDFДокумент9 страницDetection of Newcastle Disease Virus in PDFJoemar De Pascion NovillaОценок пока нет
- 2022 Article 775Документ17 страниц2022 Article 775Felipe CortesОценок пока нет
- UntitledДокумент26 страницUntitledLaura SanchezОценок пока нет
- Rabies FinalДокумент5 страницRabies FinalGINNO OSMILLOОценок пока нет
- General Introduction Into The Ebola Virus Biology and DiseaseДокумент10 страницGeneral Introduction Into The Ebola Virus Biology and DiseasewaternotaloneОценок пока нет
- Low Pathogenic Avian Influenza (LPAI)Документ9 страницLow Pathogenic Avian Influenza (LPAI)Shreeya SharmaОценок пока нет
- A Review of Bovine LeptospirosisДокумент12 страницA Review of Bovine LeptospirosisSteffanie M Clyricia NoachОценок пока нет
- Avian FluДокумент19 страницAvian FluCici Novelia ManurungОценок пока нет
- Crimean Congo Hemorrhagic FeverДокумент9 страницCrimean Congo Hemorrhagic FeverkcstincasОценок пока нет
- Lec 2 Ch3 & 4 Virus Disease in Populations and Individual AnimalsДокумент59 страницLec 2 Ch3 & 4 Virus Disease in Populations and Individual Animalsayush sainiОценок пока нет
- West Nile VirusДокумент7 страницWest Nile ViruskojerzooОценок пока нет
- Zoonoses From PoultryДокумент7 страницZoonoses From PoultryDulce AmorОценок пока нет
- World Health Organization - Swine Flu FAQ (April 26, 2009)Документ3 страницыWorld Health Organization - Swine Flu FAQ (April 26, 2009)antcomtech100% (9)
- Ebola Virus Disease: A Manual for EVD ManagementОт EverandEbola Virus Disease: A Manual for EVD ManagementMarta LadoОценок пока нет
- Asme Sec. II Part A Ed. 2013 - Sa-451 To EndДокумент1 000 страницAsme Sec. II Part A Ed. 2013 - Sa-451 To EndEnricoFurlan80% (5)
- KEYSTONE Butterfly and Rotary Valves SERIES 30,000Документ20 страницKEYSTONE Butterfly and Rotary Valves SERIES 30,000WormInchОценок пока нет
- Abpvc II Materialspart Dpropertiesmetric 140410201403 Phpapp01 PDFДокумент1 036 страницAbpvc II Materialspart Dpropertiesmetric 140410201403 Phpapp01 PDFRoger RodriguesОценок пока нет
- Steel Castings Handbook Supplement 6 PDFДокумент101 страницаSteel Castings Handbook Supplement 6 PDFjperdigon9634Оценок пока нет
- Steel Castings Handbook Supplement 6 PDFДокумент101 страницаSteel Castings Handbook Supplement 6 PDFjperdigon9634Оценок пока нет
- SCH, S9, High Alloy Data SheetsДокумент60 страницSCH, S9, High Alloy Data SheetsMiki JaksicОценок пока нет
- Steel Castings Handbook PDFДокумент41 страницаSteel Castings Handbook PDFDave ImpresoОценок пока нет
- Steel Casting Handbook Supplement 8 - High Alloy Data Sheets - Corrosion SeriesДокумент93 страницыSteel Casting Handbook Supplement 8 - High Alloy Data Sheets - Corrosion SeriesjosemiguelzuОценок пока нет
- Steel Castings Harden AbilityДокумент31 страницаSteel Castings Harden AbilityAndrei State100% (1)
- Steel Casting Handbook Supplement 8 - High Alloy Data Sheets - Corrosion SeriesДокумент93 страницыSteel Casting Handbook Supplement 8 - High Alloy Data Sheets - Corrosion SeriesjosemiguelzuОценок пока нет
- SCH, S9, High Alloy Data SheetsДокумент60 страницSCH, S9, High Alloy Data SheetsMiki JaksicОценок пока нет
- Steel Casting Handbook Supplement 8 - High Alloy Data Sheets - Corrosion SeriesДокумент93 страницыSteel Casting Handbook Supplement 8 - High Alloy Data Sheets - Corrosion SeriesjosemiguelzuОценок пока нет
- Suplement4 Steel Casting NadbookДокумент8 страницSuplement4 Steel Casting NadbookDiego Lorenzo AparicioОценок пока нет
- Steel Castings Harden AbilityДокумент31 страницаSteel Castings Harden AbilityAndrei State100% (1)
- Steel Castings Handbook Supplement 6 PDFДокумент101 страницаSteel Castings Handbook Supplement 6 PDFjperdigon9634Оценок пока нет
- Steel Castings Handbook PDFДокумент41 страницаSteel Castings Handbook PDFDave ImpresoОценок пока нет
- SCH, S9, High Alloy Data SheetsДокумент60 страницSCH, S9, High Alloy Data SheetsMiki JaksicОценок пока нет
- S 1Документ25 страницS 1Grigoris PavlakisОценок пока нет
- Evidence Over Hysteria - COVID-19 - Six Four Six Nine - MediumДокумент65 страницEvidence Over Hysteria - COVID-19 - Six Four Six Nine - MediumCody WommackОценок пока нет
- Gate XLДокумент6 страницGate XLMichael JeevaganОценок пока нет
- NCLEX RN Practice Questions 17Документ6 страницNCLEX RN Practice Questions 17RI NAОценок пока нет
- Bio Model Question Answers Souls of PandaДокумент21 страницаBio Model Question Answers Souls of PandaManoj BОценок пока нет
- Hand Book For Fish Health ManagementДокумент20 страницHand Book For Fish Health ManagementHorace Owiti O.Оценок пока нет
- For The Orthodox Faithful Who Are Confused About COVID VaccinesДокумент11 страницFor The Orthodox Faithful Who Are Confused About COVID VaccinesAleksander RizjaОценок пока нет
- MS May-2018 Paper 2 PDFДокумент16 страницMS May-2018 Paper 2 PDFMoazzem HossainОценок пока нет
- IDEXX INFLUENZA A Ab TestДокумент32 страницыIDEXX INFLUENZA A Ab TestemiliomfrОценок пока нет
- Classification of VirusesДокумент2 страницыClassification of Viruseshely shahОценок пока нет
- EncephalitisДокумент27 страницEncephalitisHasRoni Fathurrahman100% (1)
- 340 Operators ManualДокумент274 страницы340 Operators ManualAlvaro Restrepo GarciaОценок пока нет
- Exam Questions For Microboilogy, Virology 2022-2023Документ10 страницExam Questions For Microboilogy, Virology 2022-2023Amirus RussОценок пока нет
- Biology 1Документ18 страницBiology 1zaydeeeeОценок пока нет
- Endodontic Microbiology: Review of Literature: January 2011Документ14 страницEndodontic Microbiology: Review of Literature: January 2011Muhammad RaihanОценок пока нет
- Inprocess Quality Control Tests For Biological ProductsДокумент34 страницыInprocess Quality Control Tests For Biological ProductsnishathfathimaОценок пока нет
- Aquatic Sciences and Fisheries AbstractsДокумент298 страницAquatic Sciences and Fisheries AbstractsRaja DuttaОценок пока нет
- Antiviral DrugsДокумент2 страницыAntiviral DrugsEzraai HafizОценок пока нет
- CoronaviridaeДокумент9 страницCoronaviridaeiran999Оценок пока нет
- Vision Ias Science &tech Mains 365 2020Документ93 страницыVision Ias Science &tech Mains 365 2020RakeshОценок пока нет
- Virology Journal: Predicting The Subcellular Localization of Viral Proteins Within A Mammalian Host CellДокумент8 страницVirology Journal: Predicting The Subcellular Localization of Viral Proteins Within A Mammalian Host CellRuy Lopez ClosedОценок пока нет
- Pontiac Schools Pandemic Continuity Plan V - ParentДокумент14 страницPontiac Schools Pandemic Continuity Plan V - ParentAnalyn CanlasОценок пока нет
- M.sc. Applied MicrobiologyДокумент18 страницM.sc. Applied Microbiologyprism1702Оценок пока нет
- Yuvraj Priyank Marda RT-PCR ReportДокумент1 страницаYuvraj Priyank Marda RT-PCR ReportPriyank MardaОценок пока нет
- DNA VIRUSES-handout PDFДокумент11 страницDNA VIRUSES-handout PDFROTHESSA MARY CARINGALОценок пока нет
- Medical Virology Dr. Saif AL-Mayah: Rabies Virus Disease:This Virus Causes Rabies. Important PropertiesДокумент9 страницMedical Virology Dr. Saif AL-Mayah: Rabies Virus Disease:This Virus Causes Rabies. Important PropertiesAtheer AlabdyОценок пока нет