Вам также может понравиться
- CR Piopneumothoraks Nicky FIXdДокумент62 страницыCR Piopneumothoraks Nicky FIXdPutri RahmawatiОценок пока нет
- Molecular Biology Workflow Solutions BrochureДокумент62 страницыMolecular Biology Workflow Solutions BrochureJoséMaríaMoralesMuñozОценок пока нет
- Convocation ProgramДокумент125 страницConvocation ProgramZirak TayebОценок пока нет
- Referat Forensik DiatomДокумент18 страницReferat Forensik DiatomRajaAnjuPratamaPardedeОценок пока нет
- Lapsus Susp - Ca EndometriumДокумент22 страницыLapsus Susp - Ca Endometriumjeams manuОценок пока нет
- Mallory Weiss TearДокумент12 страницMallory Weiss TeararshadmunОценок пока нет
- Boys Charts Weight For Age 2 To 5 Years (Percentiles)Документ1 страницаBoys Charts Weight For Age 2 To 5 Years (Percentiles)Mimie CaliОценок пока нет
- Jurnal Reading Critical AppraisalДокумент2 страницыJurnal Reading Critical AppraisalAditya Praja'schОценок пока нет
- Editing EaДокумент43 страницыEditing EaWahyu Faisal PutraОценок пока нет
- Risk Stratification Algorithm For Orthopaedic Trauma Patients at Risk For Fat EmbolismДокумент43 страницыRisk Stratification Algorithm For Orthopaedic Trauma Patients at Risk For Fat EmbolismAravind RaviОценок пока нет
- Case Report: Urine Retention Et Causa Benign Hyperplasia ProstatДокумент37 страницCase Report: Urine Retention Et Causa Benign Hyperplasia ProstatKania A BustamОценок пока нет
- Meningitis - 2018Документ55 страницMeningitis - 2018Abraham Anaely100% (1)
- Vulnus Ictum: Dr. Jeremia SamosirДокумент64 страницыVulnus Ictum: Dr. Jeremia SamosirjerryОценок пока нет
- Guildelines For Hiv Testing NacoДокумент165 страницGuildelines For Hiv Testing NacoNagendra Singh BeniwalОценок пока нет
- Overview of Mallory - Weiss SyndromeДокумент3 страницыOverview of Mallory - Weiss SyndromeLeslyAgredaNavarroОценок пока нет
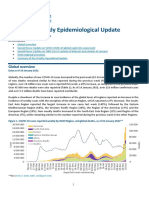
- COVID-19 Weekly Epidemiological Update: Global OverviewДокумент16 страницCOVID-19 Weekly Epidemiological Update: Global OverviewElia Nur IrmantiОценок пока нет
- Neonatal HypertensionДокумент21 страницаNeonatal HypertensionMuhammad Ammar Abdul WahabОценок пока нет
- Tennis Elbow - StatPearls - NCBI BookshelfДокумент9 страницTennis Elbow - StatPearls - NCBI BookshelfADITYA ARI HERLAMBANGОценок пока нет
- Jurnal Forensik Trauma KimiaДокумент5 страницJurnal Forensik Trauma Kimiaikram hanafiОценок пока нет
- Jurnal RubellaДокумент2 страницыJurnal RubellaAlif SpiritОценок пока нет
- Imaging of Intracranial InfectionsДокумент12 страницImaging of Intracranial Infectionsrafael rocha novaesОценок пока нет
- CombinedДокумент3 страницыCombinedSolape Akin-WilliamsОценок пока нет
- Scar Endometriosis Case Report With Literature ReviewДокумент3 страницыScar Endometriosis Case Report With Literature ReviewelsaОценок пока нет
- Toxic GasesДокумент21 страницаToxic GasesBestariNugrahiniОценок пока нет
- Efusi Pleura & EmpyemaДокумент47 страницEfusi Pleura & EmpyemaArumLaksmitaDewiОценок пока нет
- Fetal Neural Tube 2021 12 LMBR PDFДокумент24 страницыFetal Neural Tube 2021 12 LMBR PDFwayansiagaОценок пока нет
- Medel SonataДокумент54 страницыMedel Sonatamaclab macОценок пока нет
- Albumin in Liver Cirrhosis, SAДокумент37 страницAlbumin in Liver Cirrhosis, SADwinita ViviantiОценок пока нет
- OphthalmologyДокумент29 страницOphthalmologyAdebisiОценок пока нет
- Dr. I DEWA PUTU SP - PD KGer - TATALAKSANA FARMAKOLOGIK TERBARU HIPERURISEMIA DAN GOUT USIA LANJUTДокумент51 страницаDr. I DEWA PUTU SP - PD KGer - TATALAKSANA FARMAKOLOGIK TERBARU HIPERURISEMIA DAN GOUT USIA LANJUTCOVID RSHJОценок пока нет
- MedicinusДокумент64 страницыMedicinusJuandri Pia TorocozzickОценок пока нет
- Polymyalgia Rheumatica 2023Документ14 страницPolymyalgia Rheumatica 2023Carlos Alfredo Vargas Quintero100% (1)
- CH 5 Implantation, Placental Dev (Part1)Документ36 страницCH 5 Implantation, Placental Dev (Part1)Tengku Chairannisa PutriОценок пока нет
- Pembahasan CBT COMBO 3Документ802 страницыPembahasan CBT COMBO 3Sari Dewi WiratsihОценок пока нет
- KARDIOMYOPATI - Kuliah DR - ErlinaДокумент28 страницKARDIOMYOPATI - Kuliah DR - ErlinaArif Zulfian MubarokОценок пока нет
- Brugia MalayiДокумент4 страницыBrugia MalayiJericha IsidroОценок пока нет
- S31 Wood S Light in DermatologyДокумент8 страницS31 Wood S Light in DermatologyGabriel CampolinaОценок пока нет
- Arpa - 2018 0219 RaДокумент6 страницArpa - 2018 0219 Rahuseikha velayazulfahdОценок пока нет
- X - Ray Dr. Allam 2021Документ26 страницX - Ray Dr. Allam 2021little miss scare-allОценок пока нет
- E-Book Seminar PAPDI Kota Bekasi skp8Документ5 страницE-Book Seminar PAPDI Kota Bekasi skp8Miftah Nur AndamsariОценок пока нет
- Gastric Varices Management 2020Документ14 страницGastric Varices Management 2020Oscar ArdilaОценок пока нет
- Glomerular Disease - Evaluation and Differential Diagnosis in Adults - UpToDateДокумент23 страницыGlomerular Disease - Evaluation and Differential Diagnosis in Adults - UpToDateRaiya MallickОценок пока нет
- Journal Reading Pneumoni Aspirasi - Kelompok 8Документ21 страницаJournal Reading Pneumoni Aspirasi - Kelompok 8Rifly PradanaОценок пока нет
- Functional Results After Surgical Treatment For Congenital Knee DislocationДокумент8 страницFunctional Results After Surgical Treatment For Congenital Knee DislocationsarnaoushОценок пока нет
- Diabetic Ketoacidosis and Hyperosmolar Hyperglicemic Syndrome - Review BMJДокумент15 страницDiabetic Ketoacidosis and Hyperosmolar Hyperglicemic Syndrome - Review BMJJorge Flores GonzálezОценок пока нет
- Antikoagulan JurnalДокумент5 страницAntikoagulan JurnalansyemomoleОценок пока нет
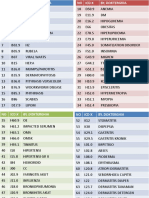
- Icd XДокумент3 страницыIcd XR Ghianesya GantinaОценок пока нет
- Jadwal-Ujian-Tpa-Program-Spesialis-Pascasarjana-Sesi-IДокумент32 страницыJadwal-Ujian-Tpa-Program-Spesialis-Pascasarjana-Sesi-IAndrio PalayukanОценок пока нет
- PemphigusДокумент32 страницыPemphigusAlondra CastilloОценок пока нет
- Chest Trauma: Annet Mary Mathew Anu Krishna Arathi.KДокумент60 страницChest Trauma: Annet Mary Mathew Anu Krishna Arathi.KAsif AbbasОценок пока нет
- Index WayneДокумент1 страницаIndex WayneAnonymous l3X3jf0NPОценок пока нет
- Case Report - Fungus BallДокумент13 страницCase Report - Fungus BallAdrian ErindraОценок пока нет
- Anemi Aplastik Dan MielodisplasiaДокумент34 страницыAnemi Aplastik Dan MielodisplasiaRoby KieranОценок пока нет
- Laporan Kasus Sindroma NefrotikДокумент13 страницLaporan Kasus Sindroma NefrotikZenithaMeidaОценок пока нет
- Anterior Resection With Low AnastomosisДокумент10 страницAnterior Resection With Low AnastomosisOhana S.Оценок пока нет
- Second AnnouncementДокумент27 страницSecond AnnouncementSheila FebrianaОценок пока нет
- Segmental Spinal Anesthesia A Systematic ReviewДокумент6 страницSegmental Spinal Anesthesia A Systematic Reviewجعفر محمدОценок пока нет
- "Otitis Media Supuratif Kronik": Case ReportДокумент20 страниц"Otitis Media Supuratif Kronik": Case ReportbagusОценок пока нет
- Case No. 55Документ33 страницыCase No. 55HovlantaОценок пока нет
- Anaest CWU OTДокумент15 страницAnaest CWU OTHana Fauzi100% (1)
- Najlaa Exam 12-03-17Документ17 страницNajlaa Exam 12-03-17Abdul SalamОценок пока нет
- Losartan Potassium 50 MG Film-Coated Tablets Losartan Potassium 100 MG Film-Coated TabletsДокумент2 страницыLosartan Potassium 50 MG Film-Coated Tablets Losartan Potassium 100 MG Film-Coated TabletsMudassar Hussain AsiОценок пока нет
- Mnemonics Psychiatric Diagnosis.Документ7 страницMnemonics Psychiatric Diagnosis.عمر الحدادОценок пока нет
- Rehabilitaion of Maxilofacial CaseДокумент56 страницRehabilitaion of Maxilofacial CasemarwaОценок пока нет
- Case-Based Discussion (CBD) Evaluation Form: Departemen Pulmonologi Dan Kedokteran RespirasiДокумент2 страницыCase-Based Discussion (CBD) Evaluation Form: Departemen Pulmonologi Dan Kedokteran RespirasiRegi SonjayaОценок пока нет
- Drug StudyДокумент5 страницDrug StudySarie LevitaОценок пока нет
- Circulatory System - Babli YadavДокумент13 страницCirculatory System - Babli YadavBabli YadavОценок пока нет
- Fnac in Tuberculous Lymphadenitis: Experience From A Tertiary Level Referral CentreДокумент6 страницFnac in Tuberculous Lymphadenitis: Experience From A Tertiary Level Referral CentreMade ChandraОценок пока нет
- Prioritization Table For The Identified Nursing ProblemsДокумент3 страницыPrioritization Table For The Identified Nursing ProblemsMia PascualОценок пока нет
- Maya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewДокумент18 страницMaya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewsukmarahastriОценок пока нет
- IV Manual 7th Edition July 2020Документ175 страницIV Manual 7th Edition July 2020Deena AlJawamisОценок пока нет
- Breast and Axilla Physical ExaminationДокумент48 страницBreast and Axilla Physical ExaminationMelissa López Hernández0% (1)
- English Task - Multiple Choices - 20200102Документ8 страницEnglish Task - Multiple Choices - 20200102bangtan's elite trashОценок пока нет
- Pediatric ShockДокумент19 страницPediatric ShockdarlingcarvajalduqueОценок пока нет
- Additional Duties of The PhlebotomistДокумент14 страницAdditional Duties of The PhlebotomistAngel Cascayan Delos SantosОценок пока нет
- Abnormality PsychologyДокумент4 страницыAbnormality PsychologyYuen-Shan LeeОценок пока нет
- CASE STUDY-Fhamitha Saara.AДокумент11 страницCASE STUDY-Fhamitha Saara.AFHAMITHAОценок пока нет
- Case Presentation IM DDHДокумент12 страницCase Presentation IM DDHAishwarya BharathОценок пока нет
- Anti-Cancer Drugs : DR Dale Srinivas University of GuyanaДокумент79 страницAnti-Cancer Drugs : DR Dale Srinivas University of Guyanamasterpiece101Оценок пока нет
- PhysiologyДокумент31 страницаPhysiologyraza20100% (1)
- Use of Alternative Medicine To Manage Pain: (CITATION Har16 /L 1033)Документ6 страницUse of Alternative Medicine To Manage Pain: (CITATION Har16 /L 1033)Syed Muhammad Baqir RazaОценок пока нет
- MORNING REPORT Ipd 040914Документ22 страницыMORNING REPORT Ipd 040914Teddy PrawiroОценок пока нет
- Homoeopathy in Breast Cancer: AbstractsДокумент5 страницHomoeopathy in Breast Cancer: Abstractskathir_cОценок пока нет
- Venous Disease: Chronic Venous Insufficiency Anatomical BackgroundДокумент16 страницVenous Disease: Chronic Venous Insufficiency Anatomical BackgroundSteve ColbertОценок пока нет
- Alternative ADHD TreatmentДокумент3 страницыAlternative ADHD TreatmentCindy VanegasОценок пока нет
- Calcarea PhosphoricaДокумент12 страницCalcarea PhosphoricaAnaSkopje100% (1)
- Assessment and Concept Map Care Plan For Critical Care PatientДокумент11 страницAssessment and Concept Map Care Plan For Critical Care Patientapi-508432180Оценок пока нет
- Case Study Endometrial PDFДокумент17 страницCase Study Endometrial PDFapi-279886264Оценок пока нет
- Traditional Chinese Dermatology: Zentral WellnessДокумент14 страницTraditional Chinese Dermatology: Zentral Wellnessan ssiОценок пока нет
- Job Shadowing PresentationДокумент8 страницJob Shadowing Presentationapi-360560383Оценок пока нет
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (81)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (29)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Оценок пока нет
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (5)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainОт EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainРейтинг: 4 из 5 звезд4/5 (95)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisОт EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisРейтинг: 5 из 5 звезд5/5 (8)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsОт EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsРейтинг: 4.5 из 5 звезд4.5/5 (6)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (59)