Вам также может понравиться
- Cooper T IUD (Par A Gard) Hormon Al IUD (Mirena) Implant Laktasi Amenorrh Ea Abstine Nce Tubekto Mi Vasekto MiДокумент5 страницCooper T IUD (Par A Gard) Hormon Al IUD (Mirena) Implant Laktasi Amenorrh Ea Abstine Nce Tubekto Mi Vasekto MiRizkia ChairaniОценок пока нет
- Intramuscular Olanzapine Versus Intramuscular Haloperidol Plus Lorazepam For The Treatment of Acute Schizopfrenia With AgitationДокумент8 страницIntramuscular Olanzapine Versus Intramuscular Haloperidol Plus Lorazepam For The Treatment of Acute Schizopfrenia With AgitationRizkia ChairaniОценок пока нет
- RetinoblastomaДокумент10 страницRetinoblastomaRizkia ChairaniОценок пока нет
- 300201Документ8 страниц300201Rido MaulanaОценок пока нет
- RetinoblastomaДокумент11 страницRetinoblastomaSyarifuddin Abdul JabbarОценок пока нет
- 2012 Data Summary NHSNДокумент19 страниц2012 Data Summary NHSNRizkia ChairaniОценок пока нет
- RetinoblastomaДокумент10 страницRetinoblastomaRizkia ChairaniОценок пока нет
- CTEVДокумент5 страницCTEVMahesa NasutionОценок пока нет
- Advances in The Management of BPHДокумент29 страницAdvances in The Management of BPHRizkia ChairaniОценок пока нет
- MRSA JournalДокумент2 страницыMRSA JournalRizkia ChairaniОценок пока нет
- Methicillin Resistant Staphylococcus AureusДокумент9 страницMethicillin Resistant Staphylococcus AureusRizkia ChairaniОценок пока нет
- MrsaДокумент6 страницMrsaRizkia ChairaniОценок пока нет
- MRSA Identification On StethoscopeДокумент48 страницMRSA Identification On StethoscopeRizkia Chairani100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Nursing Assessment and Physical ExaminationДокумент5 страницNursing Assessment and Physical ExaminationTaufik Rohman0% (1)
- Value Based Healthcare - DR Robert KaplanДокумент43 страницыValue Based Healthcare - DR Robert KaplanArin D100% (1)
- Hospital ReportДокумент29 страницHospital ReportSabinParajuliОценок пока нет
- ResumeДокумент4 страницыResumeCheranmadevi PadavettanОценок пока нет
- LingalaДокумент4 страницыLingalaFabio Ando Filho0% (1)
- Facility Planning TemplateДокумент4 страницыFacility Planning TemplateJohn Troy GamilОценок пока нет
- NCM 110 Lec Nursing Informatics Technology Part 1Документ5 страницNCM 110 Lec Nursing Informatics Technology Part 1Krizle Adaza0% (1)
- Star Health Medi Premier BrochureДокумент2 страницыStar Health Medi Premier BrochureBhaktha SinghОценок пока нет
- Design 1 Plans-ModelДокумент1 страницаDesign 1 Plans-ModelKinjal HarpavatОценок пока нет
- Shivam BuДокумент98 страницShivam BuBashu PoudelОценок пока нет
- 79360B All-On-4 Proc Prod 15.1 GBДокумент40 страниц79360B All-On-4 Proc Prod 15.1 GBRussu VadimОценок пока нет
- Medical NegligenceДокумент11 страницMedical NegligenceNimisha100% (1)
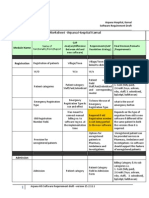
- Finalized Requirements-Worksheet - Arpana Hospital KarnalДокумент11 страницFinalized Requirements-Worksheet - Arpana Hospital KarnalMahesh PatilОценок пока нет
- The Pittston Dispatch 03-31-2013Документ60 страницThe Pittston Dispatch 03-31-2013The Times LeaderОценок пока нет
- List of Doctors Parans Update v4.0Документ9 страницList of Doctors Parans Update v4.0Franz CantaraОценок пока нет
- Menstruation BillДокумент1 страницаMenstruation BillIbrahim azeez86% (7)
- Interprofessional Collaborator Assessment Rubric: Ded By: Project FunДокумент8 страницInterprofessional Collaborator Assessment Rubric: Ded By: Project FundesiОценок пока нет
- Spinal Cord Injury Case Study (Nursing History)Документ5 страницSpinal Cord Injury Case Study (Nursing History)TobiDaОценок пока нет
- Mental Health ActДокумент9 страницMental Health ActAngelica Cassandra Villena100% (1)
- HughLaurie ST James InfirmaryДокумент7 страницHughLaurie ST James InfirmaryjoeОценок пока нет
- Hpcsa Accredited Schools PDFДокумент13 страницHpcsa Accredited Schools PDFMbalekelwa MpembeОценок пока нет
- Repair of HydroceleДокумент20 страницRepair of HydroceleNatanael AdiОценок пока нет
- Themaddoxrodtest PDFДокумент4 страницыThemaddoxrodtest PDFdechastraОценок пока нет
- Cervical RipeningДокумент7 страницCervical RipeningBagus WicaksonoОценок пока нет
- Rec To Vaginal Fistula RepairДокумент7 страницRec To Vaginal Fistula Repairnaftalina7Оценок пока нет
- Rapid Interpretation of EKG's 6th EdДокумент14 страницRapid Interpretation of EKG's 6th EdDenise De Los Reyes100% (2)
- Ound TherapyДокумент14 страницOund TherapyAndrewJohnsonJenssonОценок пока нет
- 2013 Scope of Appointment Form - CORBINДокумент2 страницы2013 Scope of Appointment Form - CORBINCorbin LindseyОценок пока нет
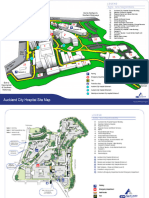
- ACH Site MapTWTДокумент2 страницыACH Site MapTWTyashacnzОценок пока нет