Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Vyom SSO Edge Data SheetДокумент2 страницыVyom SSO Edge Data SheetGiriprasad GunalanОценок пока нет
- SpringДокумент24 страницыSpringRiya IndukuriОценок пока нет
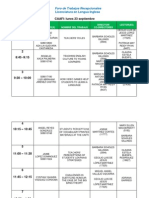
- Foro de ER - Sept - FinalThisOneДокумент5 страницForo de ER - Sept - FinalThisOneAbraham CastroОценок пока нет
- Human Resources Officer CVДокумент2 страницыHuman Resources Officer CVsreeharivzm_74762363Оценок пока нет
- Community Service Reflection PaperДокумент2 страницыCommunity Service Reflection Paperapi-525941594Оценок пока нет
- All English TensesДокумент5 страницAll English TensesIkram0% (1)
- (M2-MAIN) The Self From Various PerspectivesДокумент120 страниц(M2-MAIN) The Self From Various PerspectivesAngelo Payod100% (1)
- Table of Specification - K-12Документ15 страницTable of Specification - K-12caroline dullete77% (31)
- Harvard Divinity School, Cambridge University Press The Harvard Theological ReviewДокумент11 страницHarvard Divinity School, Cambridge University Press The Harvard Theological ReviewLuke HanscomОценок пока нет
- Perdev 2qДокумент1 страницаPerdev 2qGrace Mary Tedlos BoocОценок пока нет
- UG Unconditional Offer LetterДокумент2 страницыUG Unconditional Offer Letterzwt208961360Оценок пока нет
- 21st Century Literature From The Philippines and The World (Q1 Wk5)Документ22 страницы21st Century Literature From The Philippines and The World (Q1 Wk5)Marc Vryant De GuzmanОценок пока нет
- 8 In-Depth Quantitative Analysis QuestionsДокумент2 страницы8 In-Depth Quantitative Analysis QuestionsDeepak AhujaОценок пока нет
- HIST123 - Chapter - Church of The Immaculate Conception, SpinkhillДокумент3 страницыHIST123 - Chapter - Church of The Immaculate Conception, SpinkhillcheggОценок пока нет
- Nova Southeastern University Dissertation GuideДокумент6 страницNova Southeastern University Dissertation GuidePaperWritingServiceCheapSingapore100% (1)
- TOR EMBeD Summer 2020 InternshipДокумент2 страницыTOR EMBeD Summer 2020 InternshipvishakhaОценок пока нет
- Olivarez College: Graduate SchoolДокумент3 страницыOlivarez College: Graduate SchoolNico PelomianoОценок пока нет
- Cess Lesson 2 Sociological PerspectiveДокумент32 страницыCess Lesson 2 Sociological PerspectiveBoruto Jr CondeОценок пока нет
- 1.gilbert Et Al (Everything You Read)Документ33 страницы1.gilbert Et Al (Everything You Read)simiflorОценок пока нет
- Probability Calculation in MinesweeperДокумент2 страницыProbability Calculation in MinesweeperBrayan Perez ContrerasОценок пока нет
- Network t1 1435 1436Документ11 страницNetwork t1 1435 1436H_BioMedОценок пока нет
- Non-Nursing Theories A. Systems TheoryДокумент11 страницNon-Nursing Theories A. Systems Theoryethics wixОценок пока нет
- GRADE 8 LP 2nd RevisionДокумент3 страницыGRADE 8 LP 2nd RevisionFrezlyn ManangbaoОценок пока нет
- Cambridge Aice Marine Science SyllabusДокумент32 страницыCambridge Aice Marine Science Syllabusapi-280088207Оценок пока нет
- Collocation SДокумент2 страницыCollocation SpatykcОценок пока нет
- Agoraphobia 1Документ47 страницAgoraphobia 1We Are HanakoОценок пока нет
- Week 7 Lesson Plans 2Документ4 страницыWeek 7 Lesson Plans 2api-334646577Оценок пока нет
- Brihad-Dhatu Rupavali - TR Krishna Ma Char YaДокумент643 страницыBrihad-Dhatu Rupavali - TR Krishna Ma Char YaSatya Sarada KandulaОценок пока нет
- Ecpe TestДокумент20 страницEcpe Test09092004100% (1)
- MAPEH 9-HEALTH Learning PLANДокумент3 страницыMAPEH 9-HEALTH Learning PLANKeren B. VillalunaОценок пока нет