Вам также может понравиться
- Digestive SystemДокумент48 страницDigestive SystemJerilee SoCute WattsОценок пока нет
- SkinДокумент43 страницыSkinFhen Farrel100% (1)
- PDFДокумент64 страницыPDFJerilee SoCute WattsОценок пока нет
- Skin Diseases Disorders ConditionsДокумент104 страницыSkin Diseases Disorders ConditionsJerilee SoCute WattsОценок пока нет
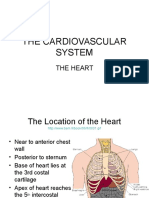
- The HeartДокумент42 страницыThe HeartJerilee SoCute WattsОценок пока нет
- Urinary SystemДокумент105 страницUrinary SystemJerilee SoCute WattsОценок пока нет
- The Circulatory System-: TransportДокумент13 страницThe Circulatory System-: TransportJerilee SoCute WattsОценок пока нет
- The Digestive System EssayДокумент3 страницыThe Digestive System EssayJerilee SoCute Watts0% (1)
- Pulmonary and Systemic CircuitsДокумент38 страницPulmonary and Systemic CircuitsJerilee SoCute WattsОценок пока нет
- The Digestive System Part 1Документ28 страницThe Digestive System Part 1Jerilee SoCute WattsОценок пока нет
- Reproductive SystemДокумент80 страницReproductive SystemJerilee SoCute WattsОценок пока нет
- The Lymphatic SystemДокумент50 страницThe Lymphatic SystemJerilee SoCute Watts100% (1)
- The Digestive System: Cont'd (From Swallowing)Документ56 страницThe Digestive System: Cont'd (From Swallowing)Jerilee SoCute WattsОценок пока нет
- Respiration System PP TДокумент57 страницRespiration System PP Troyanirudh99Оценок пока нет
- The Conducting System of The HeartДокумент37 страницThe Conducting System of The HeartJerilee SoCute WattsОценок пока нет
- Respiratory System 2Документ39 страницRespiratory System 2Jerilee SoCute WattsОценок пока нет
- Reproduction and DevelopmentДокумент53 страницыReproduction and DevelopmentJerilee SoCute WattsОценок пока нет
- Respiratory System 1Документ29 страницRespiratory System 1Jerilee SoCute WattsОценок пока нет
- Lecture 21 - Respiratory SystemДокумент59 страницLecture 21 - Respiratory SystemSkyBirdОценок пока нет
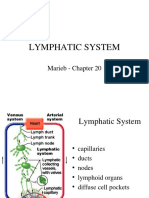
- Lymphatic System: Marieb Chapter 20Документ22 страницыLymphatic System: Marieb Chapter 20Jerilee SoCute WattsОценок пока нет
- Reproductive System DisordersДокумент62 страницыReproductive System DisordersJerilee SoCute Watts100% (2)
- Review Questions - HeartДокумент1 страницаReview Questions - HeartJerilee SoCute WattsОценок пока нет
- Respiratory Centers of The BrainДокумент36 страницRespiratory Centers of The BrainJerilee SoCute WattsОценок пока нет
- Unit 6 OsmolarityДокумент59 страницUnit 6 Osmolaritykrystal1994Оценок пока нет
- Platelets and HemostasisДокумент19 страницPlatelets and HemostasisJerilee SoCute WattsОценок пока нет
- Reproduction Summary NotesДокумент16 страницReproduction Summary NotesJerilee SoCute WattsОценок пока нет
- Human ReproductionДокумент42 страницыHuman ReproductionAliDarimiKRОценок пока нет
- Reproduction NotesДокумент20 страницReproduction NotesMario BaemamentengОценок пока нет
- Lecture 1 Cardiovascular SystemДокумент70 страницLecture 1 Cardiovascular SystemJerilee SoCute WattsОценок пока нет
- Lecture 2 Cardiovascular SystemДокумент70 страницLecture 2 Cardiovascular SystemJerilee SoCute WattsОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Chap.30 Complications From Heart Disease WordДокумент6 страницChap.30 Complications From Heart Disease WordcaisakiОценок пока нет
- A 10-Point Plan For Avoiding Hyaluronic Acid Dermal Filler-Related Complications During Facial Aesthetic Procedures and Algorithms For ManagementДокумент9 страницA 10-Point Plan For Avoiding Hyaluronic Acid Dermal Filler-Related Complications During Facial Aesthetic Procedures and Algorithms For Managementleenatalia93100% (1)
- Cognitive MedsДокумент2 страницыCognitive MedsRNStudent1100% (1)
- Counseling PhilosophyДокумент7 страницCounseling Philosophyapi-403911586Оценок пока нет
- The ARCPP 15th Annual Conference InvitationДокумент4 страницыThe ARCPP 15th Annual Conference InvitationLJ DusabanОценок пока нет
- Heavy HandsДокумент8 страницHeavy HandsPicklehead McSpazatronОценок пока нет
- Postpartum Care: Emergency SignsДокумент13 страницPostpartum Care: Emergency SignsJohnnette BedoniaОценок пока нет
- War Dogs 1Документ26 страницWar Dogs 1api-340421195Оценок пока нет
- Project ReportДокумент13 страницProject ReportRenjan Kuruvilla100% (5)
- BSHM 55 - Lesson 9 & 10Документ9 страницBSHM 55 - Lesson 9 & 10Yisu HimaaОценок пока нет
- Strabismus and Diplopia After Refractive SurgeryДокумент5 страницStrabismus and Diplopia After Refractive Surgeryyuda saputraОценок пока нет
- Case 29.07.09Документ51 страницаCase 29.07.09kanavgОценок пока нет
- Jurnal Ebm PDFДокумент10 страницJurnal Ebm PDFagustin488Оценок пока нет
- Dutch COPD Physiotherapy Guidelines PDFДокумент64 страницыDutch COPD Physiotherapy Guidelines PDFyohanОценок пока нет
- Acute Limb Ischemia: Clinical PracticeДокумент9 страницAcute Limb Ischemia: Clinical PracticeKezia TambunanОценок пока нет
- Finalpaper SchnakeДокумент6 страницFinalpaper Schnakeapi-315989347Оценок пока нет
- Sleep Apnea Research PaperДокумент9 страницSleep Apnea Research Paperaflbuagdw100% (3)
- Oncology Drills With Answers and RationalesДокумент41 страницаOncology Drills With Answers and RationalesCarol Kayas100% (1)
- Preliminary Study Evaluating Tests Used To Diagnose Canine Cranial Cruciate Ligament FailureДокумент4 страницыPreliminary Study Evaluating Tests Used To Diagnose Canine Cranial Cruciate Ligament FailureCesar AlvearОценок пока нет
- Vertigo Vertigoheel 2001Документ7 страницVertigo Vertigoheel 2001Dr. Nancy Malik100% (1)
- 6 Areas of Specialization Where Counselor WorkДокумент17 страниц6 Areas of Specialization Where Counselor WorkAaron Peñas50% (2)
- Finding Alternative ThoughtsДокумент1 страницаFinding Alternative ThoughtsOnly Probz100% (2)
- CXS Evaporated MilksДокумент4 страницыCXS Evaporated MilksVallerina TariganОценок пока нет
- Sharma Krishna N., Exploration of The History of Physiotherapy (The Scientific Research Journal of India. SRJI Vol-1 No-1 Year 2012)Документ4 страницыSharma Krishna N., Exploration of The History of Physiotherapy (The Scientific Research Journal of India. SRJI Vol-1 No-1 Year 2012)Dr. Krishna N. SharmaОценок пока нет
- Mindful Medical Practice - Clinical Narratives and Therapeutic InsightsДокумент169 страницMindful Medical Practice - Clinical Narratives and Therapeutic InsightsSkg KonОценок пока нет
- Foods That Kill CandidaДокумент3 страницыFoods That Kill Candidasexy_rusian100% (1)
- BHU Daily Stock PerformaДокумент6 страницBHU Daily Stock PerformabilalОценок пока нет
- ONLY WATCH 6th Edition 2015Документ126 страницONLY WATCH 6th Edition 2015Thimios KoukОценок пока нет
- Easy Health Insurance Claim Form PDFДокумент4 страницыEasy Health Insurance Claim Form PDFAnkithОценок пока нет
- Leg CellulitisДокумент3 страницыLeg CellulitisJessica Pacris MaramagОценок пока нет