Вам также может понравиться
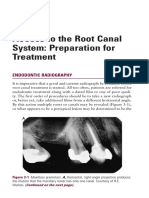
- Access To The Root Canal System: Preparation For Treatment: Endodontic RadiographyДокумент13 страницAccess To The Root Canal System: Preparation For Treatment: Endodontic RadiographyMonika LohakpureОценок пока нет
- Maxillary Anesthetic TechniquesДокумент55 страницMaxillary Anesthetic TechniquesMera Emad100% (4)
- Maxillary Injection TechniquesДокумент127 страницMaxillary Injection TechniquesD YasIr MussaОценок пока нет
- E Book BM 1Документ7 страницE Book BM 1najma byvirlianaОценок пока нет
- Maxillary Injection TechniquesДокумент129 страницMaxillary Injection Techniquesalosh60100% (1)
- Anesthetic Considerations in Dental SpecialtiesДокумент10 страницAnesthetic Considerations in Dental SpecialtiesOmar FawazОценок пока нет
- Failure of Inferior Alveolar Nerve Block: Exploring The AlternativesДокумент4 страницыFailure of Inferior Alveolar Nerve Block: Exploring The Alternativesthinkerbell_adaОценок пока нет
- Supraperiosteal or Deep Submucous InfiltrationДокумент6 страницSupraperiosteal or Deep Submucous Infiltrationbalab2311Оценок пока нет
- Local Anesthesia in Pediatric Dentistry Lecture Students 2009 MДокумент88 страницLocal Anesthesia in Pediatric Dentistry Lecture Students 2009 MIoana DănilăОценок пока нет
- Intraligamentar AnesthesiaДокумент7 страницIntraligamentar AnesthesiaGavris Bianca100% (1)
- Local Anesthesia - Nerve Blocks & ComplicationsДокумент85 страницLocal Anesthesia - Nerve Blocks & ComplicationsArchanaОценок пока нет
- Local Anesthesia Strategies For The Patient With A Hot' ToothДокумент11 страницLocal Anesthesia Strategies For The Patient With A Hot' ToothGaurav PoplaiОценок пока нет
- Update of Dental Local AnesthesiaДокумент13 страницUpdate of Dental Local AnesthesiaDeb SОценок пока нет
- Maxillary Techniques LecturesДокумент151 страницаMaxillary Techniques Lecturespeter samaanОценок пока нет
- Maxillary Techniques LecturesДокумент151 страницаMaxillary Techniques Lecturespeter samaanОценок пока нет
- 10.1007@s00784 017 2248 2Документ7 страниц10.1007@s00784 017 2248 2IndahSerafikaОценок пока нет
- Failures of Root Canal TreatmentДокумент77 страницFailures of Root Canal Treatmenthardeep kaurОценок пока нет
- Administration of Local Anaesthetic in DentistryДокумент6 страницAdministration of Local Anaesthetic in DentistryridaОценок пока нет
- Gow Gates Nerve BlockДокумент4 страницыGow Gates Nerve BlockHudh HudОценок пока нет
- Epidural AnalgesiaДокумент16 страницEpidural AnalgesiaspreeasОценок пока нет
- Greater Palatine Nerve BlockДокумент3 страницыGreater Palatine Nerve BlockEcho WhyОценок пока нет
- Evaluation of Local Anaesthetic Failures in Dental PracticeДокумент6 страницEvaluation of Local Anaesthetic Failures in Dental PracticenrlОценок пока нет
- Maxillaary AnesthesiaДокумент44 страницыMaxillaary AnesthesiaAlex HaileyesusОценок пока нет
- Hematoma by PSAДокумент5 страницHematoma by PSAMouy EngОценок пока нет
- Hot Tooth ManagementДокумент21 страницаHot Tooth Managementwu yuoОценок пока нет
- X-Tip Intraosseous Injection System As A Primary Anesthesia For Irreversible Pulpitis of Posterior Mandibular Teeth A Randomized Clinical TrailДокумент8 страницX-Tip Intraosseous Injection System As A Primary Anesthesia For Irreversible Pulpitis of Posterior Mandibular Teeth A Randomized Clinical TrailLeticia RiveraОценок пока нет
- Orim 36 05 401 407Документ7 страницOrim 36 05 401 407Neil SchembriОценок пока нет
- Anesthetic Technique For Inferior Alveolar Nerve Block: A New ApproachДокумент5 страницAnesthetic Technique For Inferior Alveolar Nerve Block: A New ApproachMaqbul AlamОценок пока нет
- Local Anaesthetics in Dentistry: A SeriesДокумент4 страницыLocal Anaesthetics in Dentistry: A SeriesCarlos Valera MtzОценок пока нет
- Greater PalatineДокумент41 страницаGreater Palatinekaran patelОценок пока нет
- Amsa (Anterior Middle Superior Alveolar) Injection: A Boon To Maxillaryperiodontal SurgeryДокумент5 страницAmsa (Anterior Middle Superior Alveolar) Injection: A Boon To Maxillaryperiodontal SurgerysetoОценок пока нет
- CLOI Kmmereretal.2017 ILAIANBExtractionsДокумент8 страницCLOI Kmmereretal.2017 ILAIANBExtractionsRohma DwiОценок пока нет
- Broken Local Anesthetic NeedlesДокумент5 страницBroken Local Anesthetic NeedlesGina CastilloОценок пока нет
- Clinical: Dental Pulp Neurophysiology: Part 1. Clinical and Diagnostic ImplicationsДокумент5 страницClinical: Dental Pulp Neurophysiology: Part 1. Clinical and Diagnostic ImplicationsSiddharth DhanarajОценок пока нет
- Bilateral Sagittal Split OsteotomyДокумент8 страницBilateral Sagittal Split OsteotomydoctorniravОценок пока нет
- Anesth-Lab (Local Anesthesia)Документ7 страницAnesth-Lab (Local Anesthesia)Marrion Jules Sequitin MendozaОценок пока нет
- SpixДокумент6 страницSpixAlienformoflifeОценок пока нет
- Simple Technique For Lip and Nasolabial Fold Anesthesia For Injectable FillersДокумент3 страницыSimple Technique For Lip and Nasolabial Fold Anesthesia For Injectable FillersGina CastilloОценок пока нет
- ArthrocentesisДокумент4 страницыArthrocentesisAlejandro RuizОценок пока нет
- ENDODONTIC PAIN MANAGEMENT - Pro - Dr. Mitul JoshiДокумент68 страницENDODONTIC PAIN MANAGEMENT - Pro - Dr. Mitul Joshiخالد الجدياويОценок пока нет
- Gow Gates1973Документ8 страницGow Gates1973Sri RaamОценок пока нет
- 14 Techniques of Mandibular AnesthesiaДокумент27 страниц14 Techniques of Mandibular Anesthesiaapi-3711066100% (7)
- Systematic Review On Sucess of Narrow-Diameter Dental ImplantsДокумент37 страницSystematic Review On Sucess of Narrow-Diameter Dental ImplantsMaryGonzalesʚïɞОценок пока нет
- Influence of Buccal Segment Size On Prevention of Side Effects From Incisor IntrusionДокумент8 страницInfluence of Buccal Segment Size On Prevention of Side Effects From Incisor IntrusionAly OsmanОценок пока нет
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentОт EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentОценок пока нет
- Trephination For AcuteДокумент3 страницыTrephination For AcuteDr.Ibrahim Al-QwizanyОценок пока нет
- ENGanesthesiamanndibleДокумент48 страницENGanesthesiamanndibleRoxanaAnaHociungОценок пока нет
- Presentation 1Документ46 страницPresentation 1anamiqbalОценок пока нет
- Anesthetic Technique For Inferior Alveolar Nerve Block: A New ApproachДокумент5 страницAnesthetic Technique For Inferior Alveolar Nerve Block: A New ApproachIonela AlexandraОценок пока нет
- Injection Pterygomandibular: EvaluationДокумент5 страницInjection Pterygomandibular: EvaluationMaqbul AlamОценок пока нет
- Inferior Alveolar TechniqueДокумент8 страницInferior Alveolar Techniquebalab2311Оценок пока нет
- PDLInjection Malamed OOO1982Документ5 страницPDLInjection Malamed OOO1982iulian tigauОценок пока нет
- Techniques of Local Anesthesia: Jimma University. Dentistry DepartemntДокумент108 страницTechniques of Local Anesthesia: Jimma University. Dentistry DepartemntEthiopia TekdemОценок пока нет
- Evaluation of New Injection and Cavity Preparation Model in Local Anesthesia TeachingДокумент8 страницEvaluation of New Injection and Cavity Preparation Model in Local Anesthesia TeachingBagis Emre GulОценок пока нет
- Complication & Failure of ImplantsДокумент82 страницыComplication & Failure of ImplantsDrIbrahimShaikhОценок пока нет
- IntJOralHealthDent 8-3-256 258Документ3 страницыIntJOralHealthDent 8-3-256 258MutiaRamadhantiiОценок пока нет
- Anesthesia Quiz With ReferencesДокумент16 страницAnesthesia Quiz With ReferencesfrancisОценок пока нет
- A Comparison of Periodontal Intraligamental Anesthesia Using Etidocaine HCI and Lidocaine HCIДокумент4 страницыA Comparison of Periodontal Intraligamental Anesthesia Using Etidocaine HCI and Lidocaine HCITeremfMoraОценок пока нет
- Apical Terminus Location of Root Canal Treatment ProceduresДокумент5 страницApical Terminus Location of Root Canal Treatment ProceduresbubuvulpeaОценок пока нет
- NBDE Remembered 2 New YorkДокумент242 страницыNBDE Remembered 2 New YorkR MОценок пока нет
- Bioenergetics and Biological Oxidation FinalДокумент27 страницBioenergetics and Biological Oxidation Finalapi-19859346Оценок пока нет
- Physioex Lab Report: Pre-Lab Quiz ResultsДокумент3 страницыPhysioex Lab Report: Pre-Lab Quiz ResultsNicole de LeonОценок пока нет
- %pecta (: P'erfectedДокумент5 страниц%pecta (: P'erfectedjuan perez arrikitaunОценок пока нет
- Jaw RelationДокумент48 страницJaw RelationBharanija100% (1)
- MODUL Praktikum Anatomi Dan HistologiДокумент20 страницMODUL Praktikum Anatomi Dan HistologiandikaОценок пока нет
- Perfusionist Job DescriptionДокумент3 страницыPerfusionist Job DescriptionNouman IshaqОценок пока нет
- TCM Student Study GuideДокумент40 страницTCM Student Study GuideHomework PingОценок пока нет
- 15-Lead ECG PowerpointДокумент20 страниц15-Lead ECG Powerpointgillian102290Оценок пока нет
- LeafanatomyДокумент18 страницLeafanatomyTeach FrezОценок пока нет
- Organic AcidsДокумент25 страницOrganic Acidssatti_indianОценок пока нет
- Reports 2Документ10 страницReports 2Tejaswini ReddyОценок пока нет
- Breathing Exercises 0Документ2 страницыBreathing Exercises 0Julyhathul Kuraishi100% (1)
- Biomechanics in Applications PDFДокумент424 страницыBiomechanics in Applications PDFRAUL EDUARDO GUTIERREZ COITIÑO100% (1)
- Gbio 2122 Week 1 10 by Kuya CharlesДокумент18 страницGbio 2122 Week 1 10 by Kuya CharlesChoe Yoek Soek100% (2)
- Nursing Exam CompreДокумент9 страницNursing Exam ComprerikidbОценок пока нет
- Analiza Haplo Grupa Bosnjaka I Dr.Документ12 страницAnaliza Haplo Grupa Bosnjaka I Dr.damirzeОценок пока нет
- CHAPTER 2 - Textbook ExerciseДокумент8 страницCHAPTER 2 - Textbook ExerciseLeena HingОценок пока нет
- FLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeДокумент3 страницыFLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAizaz ul HaqОценок пока нет
- KGMU B.SC Nursing Entrance Exam Bilology Previous Year PaperДокумент8 страницKGMU B.SC Nursing Entrance Exam Bilology Previous Year PaperTech GaminggОценок пока нет
- MICROBIOLOGY - Microbial Taxonomy, Cell Structure and Bacterial Metabolism, Growth & GeneticsДокумент16 страницMICROBIOLOGY - Microbial Taxonomy, Cell Structure and Bacterial Metabolism, Growth & GeneticsRobie LeañoОценок пока нет
- Enteric Nervous SystemДокумент12 страницEnteric Nervous SystemedgarОценок пока нет
- The Endocrine System: Year 9 Biological ScienceДокумент20 страницThe Endocrine System: Year 9 Biological ScienceSasha VoleskyОценок пока нет
- 8 Cell - The Unit of Life-NotesДокумент6 страниц8 Cell - The Unit of Life-NotesBhavanya RavichandrenОценок пока нет
- Background Results: DR Aditya Bhat, DR, Amit Misri Department of Paediatric Cardiology, Medanta-The Medicity, GurgaonДокумент1 страницаBackground Results: DR Aditya Bhat, DR, Amit Misri Department of Paediatric Cardiology, Medanta-The Medicity, GurgaonADОценок пока нет
- Biology For CAPE Unit 1 Chapter 12 AnswersДокумент8 страницBiology For CAPE Unit 1 Chapter 12 AnswersFiveLimaRomeoОценок пока нет
- Digestion Test BiologyДокумент3 страницыDigestion Test BiologyKatrīna SimanovskaОценок пока нет
- English IIДокумент107 страницEnglish IIlauroОценок пока нет
- Patel 2014Документ7 страницPatel 2014Javiera Munizaga MuñozОценок пока нет
- Sbk3023 Food Science and NutritionДокумент20 страницSbk3023 Food Science and NutritionKuMohdSyafiqОценок пока нет
- Davis's NCLEX-RN® Success 3E (2012) - MEMORY AIDS - IMPORTANTДокумент4 страницыDavis's NCLEX-RN® Success 3E (2012) - MEMORY AIDS - IMPORTANTMaria Isabel Medina MesaОценок пока нет