Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Sparks and Taylor's Nursing Diagnosis Pocket GuideДокумент514 страницSparks and Taylor's Nursing Diagnosis Pocket GuideShawnPoirier100% (13)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- OSCE Checklist: Thyroid Status ExaminationДокумент2 страницыOSCE Checklist: Thyroid Status ExaminationNur Farhana Athirah Azhari100% (2)
- Test BДокумент11 страницTest BMaria HillОценок пока нет
- 123456789-Lectures On Homoeopathic Philosophy by JT Kent-123456789Документ181 страница123456789-Lectures On Homoeopathic Philosophy by JT Kent-123456789fapatel95Оценок пока нет
- Nursing Health HistoryДокумент11 страницNursing Health Historyrubycorazon_edizaОценок пока нет
- Edison College Nursing Program Infection Risk PlanДокумент3 страницыEdison College Nursing Program Infection Risk PlanBrian Bracher93% (43)
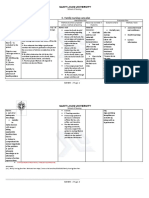
- C. Family Nursing Care Plan: Saint Louis UniversityДокумент2 страницыC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- OSCE ManualДокумент40 страницOSCE Manualdkasis100% (1)
- Nursing Care Plan for Respiratory IssuesДокумент10 страницNursing Care Plan for Respiratory IssuesMykel Jake VasquezОценок пока нет
- Wrist Sizing HamiltonДокумент3 страницыWrist Sizing HamiltondonkeyendutОценок пока нет
- Wrist Sizing Hamilton PDFДокумент3 страницыWrist Sizing Hamilton PDFdonkeyendutОценок пока нет
- Ap 1 PDFДокумент7 страницAp 1 PDFdonkeyendutОценок пока нет
- Analisa Dan Penanganan Hepatitis Kemenkes RIДокумент8 страницAnalisa Dan Penanganan Hepatitis Kemenkes RIIzzi FekratОценок пока нет
- Dep 1 PDFДокумент11 страницDep 1 PDFdonkeyendutОценок пока нет
- Standardized Mini-Mental State Exam GuideДокумент2 страницыStandardized Mini-Mental State Exam GuideSummer WrightОценок пока нет
- Mekanisme Aksi DopaminДокумент14 страницMekanisme Aksi DopamindonkeyendutОценок пока нет
- Dopamin 2 PDFДокумент8 страницDopamin 2 PDFdonkeyendutОценок пока нет
- Gold WR 06Документ100 страницGold WR 06Melissa VidalesОценок пока нет
- Fatique and Artritis Psoriatic PDFДокумент72 страницыFatique and Artritis Psoriatic PDFdonkeyendutОценок пока нет
- Depression Theory PDFДокумент2 страницыDepression Theory PDFdonkeyendutОценок пока нет
- Looking Beyond The Monoamine Hypothesis: Johan A Den BoerДокумент9 страницLooking Beyond The Monoamine Hypothesis: Johan A Den BoerdonkeyendutОценок пока нет
- HHLДокумент7 страницHHLdonkeyendutОценок пока нет
- Jurnal Geriatri Editorial - Dementia.npsДокумент5 страницJurnal Geriatri Editorial - Dementia.npsdonkeyendutОценок пока нет
- How To Measure Cd14Документ38 страницHow To Measure Cd14donkeyendutОценок пока нет
- Summary Sepsis ManagementДокумент60 страницSummary Sepsis ManagementdonkeyendutОценок пока нет
- Tabel Dan Grafik Psiko ACPM 2014Документ1 страницаTabel Dan Grafik Psiko ACPM 2014donkeyendutОценок пока нет
- Turgor KulitДокумент21 страницаTurgor KulitChairunisa AnggrainiОценок пока нет
- Tesis Lampiran 9Документ5 страницTesis Lampiran 9donkeyendutОценок пока нет
- Jurnal Geriatri Eur Geriatr Med 2015Документ6 страницJurnal Geriatri Eur Geriatr Med 2015donkeyendutОценок пока нет
- Jurnal Geriatri Int J Geriatr Psychiatry 2014Документ9 страницJurnal Geriatri Int J Geriatr Psychiatry 2014donkeyendutОценок пока нет
- Jurnal 1 Impaired Tcell in HIVДокумент9 страницJurnal 1 Impaired Tcell in HIVdonkeyendutОценок пока нет
- Occupational Asthma Occupational Asthma: Sri Handayani LubisДокумент19 страницOccupational Asthma Occupational Asthma: Sri Handayani LubisdonkeyendutОценок пока нет
- Tesis Lampiran Tabel Induk RevisiДокумент1 страницаTesis Lampiran Tabel Induk RevisidonkeyendutОценок пока нет
- Jurnal 11 CD Manual Anthrax May2012Документ4 страницыJurnal 11 CD Manual Anthrax May2012donkeyendutОценок пока нет
- Dr. Hendra Ajbr0001-0175Документ15 страницDr. Hendra Ajbr0001-0175donkeyendutОценок пока нет
- Baru Anthrax - Protocol PDFДокумент13 страницBaru Anthrax - Protocol PDFdonkeyendutОценок пока нет
- Nakamura 2008 Critical CareДокумент2 страницыNakamura 2008 Critical CaredonkeyendutОценок пока нет
- Infliximab (Remicade) in The Treatment of Psoriatic ArthritisДокумент12 страницInfliximab (Remicade) in The Treatment of Psoriatic ArthritisdonkeyendutОценок пока нет
- Ap 1Документ7 страницAp 1donkeyendutОценок пока нет
- Wound Essentials 5 Investigating Wound InfectionДокумент5 страницWound Essentials 5 Investigating Wound Infectionyash agarwalОценок пока нет
- Peads Teacher MannualДокумент108 страницPeads Teacher MannualMobin Ur Rehman KhanОценок пока нет
- Pre-Op Deep BreathingДокумент8 страницPre-Op Deep BreathingEmmanuel BeresoОценок пока нет
- Nursing Care Plan for Post-Surgical ClientДокумент5 страницNursing Care Plan for Post-Surgical ClientQueen Shine0% (1)
- Format of Case Study-121Документ4 страницыFormat of Case Study-121Shaina OturdoОценок пока нет
- Heyer Vizor Cs - Manual 1.0 enДокумент68 страницHeyer Vizor Cs - Manual 1.0 enkalandorka92Оценок пока нет
- Neonatal Pneumonia in Rural Bangladesh: Prevalence, Clinical Features and OutcomesДокумент5 страницNeonatal Pneumonia in Rural Bangladesh: Prevalence, Clinical Features and Outcomesmirashabrina12Оценок пока нет
- Patient Care Conference: Small Group Teaching MethodДокумент3 страницыPatient Care Conference: Small Group Teaching MethodValarmathiОценок пока нет
- Pneumosinus Dilatans Frontalis: A Case ReportДокумент5 страницPneumosinus Dilatans Frontalis: A Case ReportInternational Medical PublisherОценок пока нет
- NCPДокумент17 страницNCPShayne Jessemae AlmarioОценок пока нет
- Case Study CholelithiasisДокумент2 страницыCase Study CholelithiasisJes SarylОценок пока нет
- 664717ku PDFДокумент19 страниц664717ku PDFShankar Sex boyОценок пока нет
- Clinical Evidence for Diagnosing Chronic Heart FailureДокумент209 страницClinical Evidence for Diagnosing Chronic Heart Failurerahma watiОценок пока нет
- Performance of Clinical Signs in Diagnosing DehydrationДокумент13 страницPerformance of Clinical Signs in Diagnosing DehydrationAncuk RaimuОценок пока нет
- Signs and Symptoms of Pancreatic Cancer Fact Sheet Dec 2014Документ6 страницSigns and Symptoms of Pancreatic Cancer Fact Sheet Dec 2014Nus EuОценок пока нет
- Nursing Case StudyДокумент10 страницNursing Case StudyAriel Vincent G. YeeОценок пока нет
- Nutrition Intervention Case StudiesДокумент8 страницNutrition Intervention Case StudiesSammy OhОценок пока нет
- Compiled DocumentДокумент261 страницаCompiled DocumentAbhigyan Kishor100% (1)
- Casumpang V CortejoДокумент12 страницCasumpang V CortejoMariel CabubunganОценок пока нет
- Solving Safety Implications in A Case Based Decision-Support System in MedicineДокумент81 страницаSolving Safety Implications in A Case Based Decision-Support System in MedicineClo SerОценок пока нет
- Reflective Writing #1 First Week in Clinical PlacementДокумент1 страницаReflective Writing #1 First Week in Clinical PlacementShrests SinhaОценок пока нет