Вам также может понравиться
- Feb 2014 FinalДокумент2 страницыFeb 2014 Finalks2Оценок пока нет
- SF Application 2013Документ4 страницыSF Application 2013ks2Оценок пока нет
- Diclegis Full Prescribing InformationДокумент12 страницDiclegis Full Prescribing Informationks2Оценок пока нет
- IBM Software SupportДокумент4 страницыIBM Software Supportks2Оценок пока нет
- India: Photo Adven TuresДокумент1 страницаIndia: Photo Adven Turesks2Оценок пока нет
- Understanding DB2 Bufferpool Tuning 2005 FinalДокумент40 страницUnderstanding DB2 Bufferpool Tuning 2005 Finalks2Оценок пока нет
- Norton 360 $25 Upgrade RebateДокумент1 страницаNorton 360 $25 Upgrade Rebateks2Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- MedicalДокумент124 страницыMedicalJuju_Amar100% (1)
- Cardiopulmonary BypassДокумент42 страницыCardiopulmonary BypassСергей МатюшинОценок пока нет
- Ahmed Thesis Surgery 2018Документ84 страницыAhmed Thesis Surgery 2018fedhawakОценок пока нет
- Epic InstructionsДокумент3 страницыEpic Instructionserik_romanelliОценок пока нет
- Sanjivani Anesthesia RecordДокумент4 страницыSanjivani Anesthesia RecordAdvait KarmarkarОценок пока нет
- Dilation and CurettageДокумент8 страницDilation and CurettageMelody B. Miguel100% (1)
- Congenital Diaphragmatic HerniaДокумент29 страницCongenital Diaphragmatic Herniapaddy9980Оценок пока нет
- General AnaesthesiaДокумент24 страницыGeneral AnaesthesiaIrika100% (1)
- LA Systemic Toxicity Current PerspectiveДокумент10 страницLA Systemic Toxicity Current PerspectiveGeetha SoundaryaОценок пока нет
- Services Marketing "Shouldice Hospital Limited" - Case SubmissionДокумент6 страницServices Marketing "Shouldice Hospital Limited" - Case SubmissionVenkata Sai Pavan JeerlaОценок пока нет
- Surgery Written Assignment2016Документ2 страницыSurgery Written Assignment2016Tyler EmmendorferОценок пока нет
- Ctet Jan 2012 Paper 1 Eng 2Документ7 страницCtet Jan 2012 Paper 1 Eng 2SureshkumaryadavОценок пока нет
- Inhalation AnestheticsДокумент29 страницInhalation AnestheticsIta RositaОценок пока нет
- Pharmacology: Learning PlanДокумент12 страницPharmacology: Learning PlanMelanie GaledoОценок пока нет
- 4610 40 V1 0 0 Ralma TXT PDFДокумент158 страниц4610 40 V1 0 0 Ralma TXT PDFJean Carlos FlorianoОценок пока нет
- MDK Products Catalogue 2022.9.30Документ17 страницMDK Products Catalogue 2022.9.30Medis MEDISОценок пока нет
- Preboard Exam D - Test 3: Medical Surgical Nursing Exam: Answers & RationaleДокумент11 страницPreboard Exam D - Test 3: Medical Surgical Nursing Exam: Answers & RationaleHasan A AsFourОценок пока нет
- PREPUMASTERKEY (Repaired)Документ2 031 страницаPREPUMASTERKEY (Repaired)surviving nursing schoolОценок пока нет
- Sargical Safety ProjectДокумент18 страницSargical Safety ProjectKeshava Nagalkar100% (1)
- Pharmacology Whole Imp Points Ploaded by Hafiz BilalДокумент22 страницыPharmacology Whole Imp Points Ploaded by Hafiz BilalALI HASSANОценок пока нет
- Medical Terminology and PhrasesДокумент60 страницMedical Terminology and Phrasesapi-3743320Оценок пока нет
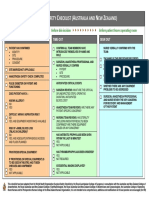
- LST 2009 Surgical Safety Check List (Australia and New Zealand) PDFДокумент1 страницаLST 2009 Surgical Safety Check List (Australia and New Zealand) PDFaskjhwiuehОценок пока нет
- Cardiac Anesthesia - Made Ridiculously Simple by Art Wallace, M.D., PH.DДокумент17 страницCardiac Anesthesia - Made Ridiculously Simple by Art Wallace, M.D., PH.Dstanwalks100% (1)
- Typhon Case LogДокумент3 страницыTyphon Case LogJeremy HallОценок пока нет
- 7 Principles of Uncomplicated ExodontiaДокумент43 страницы7 Principles of Uncomplicated Exodontiaray774432Оценок пока нет
- Dissertation Topics in Cardiac AnaesthesiaДокумент5 страницDissertation Topics in Cardiac AnaesthesiaDoMyPapersMilwaukee100% (1)
- 25A RA Changing Anaesthesia TrendsДокумент4 страницы25A RA Changing Anaesthesia TrendstomeyttoОценок пока нет
- Aid To Multiple Choice Questions in Surgery 20161013Документ166 страницAid To Multiple Choice Questions in Surgery 20161013Cheng Xinvenn100% (1)
- 112 Prone PositioningДокумент6 страниц112 Prone PositioningMade Septyana Parama AdiОценок пока нет
- Infiltration Anaesthesia For Tympanoplasty: A Comparison of Dexmedetomidine and Clonidine As Adjuvants To Lignocaine and AdrenalineДокумент7 страницInfiltration Anaesthesia For Tympanoplasty: A Comparison of Dexmedetomidine and Clonidine As Adjuvants To Lignocaine and AdrenalineIJAR JOURNALОценок пока нет