Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Skin Wounds ClassificationsДокумент66 страницSkin Wounds ClassificationsLaoShiYuОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Basic Dribbling For 4 Yr. Olds and UpДокумент8 страницBasic Dribbling For 4 Yr. Olds and UpLaoShiYuОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Music RulesДокумент6 страницMusic RulesLaoShiYuОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Psycho Social TheoryДокумент27 страницPsycho Social TheoryLaoShiYuОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Basketball Games, Skills & DrillsДокумент12 страницBasketball Games, Skills & DrillsswaggerboxОценок пока нет
- Just BuggyДокумент20 страницJust BuggyLaoShiYuОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Christmas TreeДокумент2 страницыChristmas TreeLaoShiYuОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- An Activity To Practice Reading Rhythms.: Created by Tami MangussoДокумент7 страницAn Activity To Practice Reading Rhythms.: Created by Tami MangussoLaoShiYuОценок пока нет
- JurnalДокумент12 страницJurnalLaoShiYuОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Daya Tahan KardiovaskularДокумент33 страницыDaya Tahan KardiovaskularLaoShiYuОценок пока нет
- Froggy BeatsДокумент15 страницFroggy BeatsLaoShiYuОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Presentation 1Документ13 страницPresentation 1LaoShiYuОценок пока нет
- ElpДокумент19 страницElpLaoShiYuОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Child Abuse 2Документ8 страницChild Abuse 2LaoShiYuОценок пока нет
- What Is The Sport You Like MostДокумент1 страницаWhat Is The Sport You Like MostLaoShiYuОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Active and Passive Voice p1Документ26 страницActive and Passive Voice p1LaoShiYuОценок пока нет
- Ang Yee Hui Ruth Yu Len Ai Sharon Wong Xue RouДокумент13 страницAng Yee Hui Ruth Yu Len Ai Sharon Wong Xue RouLaoShiYuОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Narrative Essay About EventДокумент9 страницNarrative Essay About EventLaoShiYuОценок пока нет
- MindmapДокумент2 страницыMindmapLaoShiYuОценок пока нет
- CTNeoBC Pooled AnalysisДокумент9 страницCTNeoBC Pooled AnalysistabaresgonzaloОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- SMA Advanced Sports Taping Presentation DSR Handouts PDFДокумент4 страницыSMA Advanced Sports Taping Presentation DSR Handouts PDFHamada Said AliОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- NCM 100 Carpers Pattern of KnowingДокумент16 страницNCM 100 Carpers Pattern of KnowingconinitasОценок пока нет
- Patient Information: Corp.: Bill To:: Doc. No: LPL/CLC/QF/2806Документ1 страницаPatient Information: Corp.: Bill To:: Doc. No: LPL/CLC/QF/2806TarunОценок пока нет
- Mentored by Nature: Bradley L. JonesДокумент5 страницMentored by Nature: Bradley L. JonesAlfredo RamzОценок пока нет
- Dha 022019 PDFДокумент20 страницDha 022019 PDFDrNishchitha K100% (2)
- Updates in The Management of Diabetic Ketoacidosis: Kathryn Evans Kreider, DNP, FNP-BCДокумент7 страницUpdates in The Management of Diabetic Ketoacidosis: Kathryn Evans Kreider, DNP, FNP-BCLenin Zavaleta RodriguezОценок пока нет
- Iggy Med Surg Test Bank Chapter 007Документ10 страницIggy Med Surg Test Bank Chapter 007Tracy Bartell100% (5)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Gastroesophageal Reflux DiseaseДокумент9 страницGastroesophageal Reflux DiseaseNicole Tupayachi ArceОценок пока нет
- Nursing Care and Do-Not-Resuscitate (DNR) Decisions: PurposeДокумент6 страницNursing Care and Do-Not-Resuscitate (DNR) Decisions: PurposeBea-ayesha A. PandaoОценок пока нет
- Final Period - Assignment NCM 105Документ3 страницыFinal Period - Assignment NCM 105Chester NicoleОценок пока нет
- Guidelines To Evaluation of Permanent ImpairmentДокумент73 страницыGuidelines To Evaluation of Permanent ImpairmentMarco Antonio Borges das NevesОценок пока нет
- Nursing Care Plan Clubfoot or Talipes EquinovarusДокумент6 страницNursing Care Plan Clubfoot or Talipes EquinovarusMarzie LugtuОценок пока нет
- 20th Century NurseДокумент5 страниц20th Century NurseMisch Yeen100% (1)
- Trauma BrotraumaДокумент2 страницыTrauma BrotraumaSri WiadnyaniОценок пока нет
- Nursing Responsibilities For Oxygen AdministrationДокумент3 страницыNursing Responsibilities For Oxygen AdministrationJahseh WolfeОценок пока нет
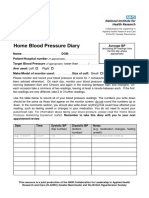
- Home Blood Pressure DiaryДокумент2 страницыHome Blood Pressure DiaryCherieОценок пока нет
- Local Anesthesia Exam TipsДокумент9 страницLocal Anesthesia Exam TipsshadapaaakОценок пока нет
- Nxlex 6Документ50 страницNxlex 6Arvin CamposОценок пока нет
- Surgical SafetyДокумент23 страницыSurgical SafetyNimi BatuboОценок пока нет
- Medial Knee Pain Treatment Using Secondary VesselsДокумент6 страницMedial Knee Pain Treatment Using Secondary Vesselskeiraku100% (3)
- A Critical Analysis of SchizophreniaДокумент5 страницA Critical Analysis of Schizophreniaapi-283426681Оценок пока нет
- Solving Math Word Problems: Steps Tips For Success ExampleДокумент3 страницыSolving Math Word Problems: Steps Tips For Success ExampleDhiman NathОценок пока нет
- PIID 184 Post Mortem April 17Документ7 страницPIID 184 Post Mortem April 17Rey Loro PongautanОценок пока нет
- Hospital Design GuidelinesДокумент33 страницыHospital Design GuidelinesRohit Gupta100% (3)
- Prosto FixДокумент3 страницыProsto FixNiken Tri HapsariОценок пока нет
- Case Study PcosДокумент6 страницCase Study Pcosapi-315331895Оценок пока нет
- Modified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2Документ9 страницModified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2indirinoor5Оценок пока нет
- Terri Campbell MAДокумент2 страницыTerri Campbell MAapi-121348673Оценок пока нет
- Chapter 6 NeuroemergencyДокумент21 страницаChapter 6 NeuroemergencyEdo FebrianОценок пока нет
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (1)