Вам также может понравиться
- Muscular System Chapter Test ReviewДокумент6 страницMuscular System Chapter Test ReviewLynda Obi100% (2)
- 2011 Scapulothoracic and Scapulohumeral Exercises, A Narrative Review of Electromyographic StudiesДокумент13 страниц2011 Scapulothoracic and Scapulohumeral Exercises, A Narrative Review of Electromyographic StudiesDiego SubiabreОценок пока нет
- Serdev Suture Techniques Breast Lift - Prof Nikolay P Serdev MD PHDДокумент4 страницыSerdev Suture Techniques Breast Lift - Prof Nikolay P Serdev MD PHDjobetobaОценок пока нет
- Corrective Exercise GuideДокумент13 страницCorrective Exercise GuideKetsmy Desrosiers100% (1)
- Bowflex Xtreme 2 SE Home Gym ManualДокумент92 страницыBowflex Xtreme 2 SE Home Gym ManualBest Home Gym100% (1)
- Upper Limb McqsДокумент48 страницUpper Limb McqsFarhad Ali100% (2)
- Muscle Stretching in Manual Therapy I - The Extremities (Team Nanban) (TPB)Документ177 страницMuscle Stretching in Manual Therapy I - The Extremities (Team Nanban) (TPB)CNPOULIS100% (22)
- Aesthetic and Reconstructive Breast Surgery - Solving Complications and Avoiding Unfavorable Results PDFДокумент222 страницыAesthetic and Reconstructive Breast Surgery - Solving Complications and Avoiding Unfavorable Results PDFAhmed Attia100% (1)
- Anatomy Mnemonics 2Документ50 страницAnatomy Mnemonics 2Nourhan JamalОценок пока нет
- Rehabilitation For Shoulder Instability - Current PDFДокумент15 страницRehabilitation For Shoulder Instability - Current PDFmariaОценок пока нет
- Rehabilitation of Shoulder Impingement Syndrome and Rotator Cuff Injuries: An Evidence-Based ReviewДокумент10 страницRehabilitation of Shoulder Impingement Syndrome and Rotator Cuff Injuries: An Evidence-Based ReviewEduardo Santana SuárezОценок пока нет
- Chapter 6: Spine and Spinal Cord Trauma ObjectivesДокумент23 страницыChapter 6: Spine and Spinal Cord Trauma ObjectivesfadhillahilmayantiОценок пока нет
- Shoulder-Acromioclavicular Separation PDFДокумент13 страницShoulder-Acromioclavicular Separation PDFFebrian ParuraОценок пока нет
- PLC InjuryДокумент5 страницPLC InjuryTeng HanОценок пока нет
- The Terrible Triad of The ElbowДокумент5 страницThe Terrible Triad of The Elbowapi-250084607Оценок пока нет
- SHOULDER INSTABILITY ManagДокумент18 страницSHOULDER INSTABILITY ManagFarhan JustisiaОценок пока нет
- Badri 2018Документ6 страницBadri 2018pakemainmainОценок пока нет
- Research FinalДокумент36 страницResearch FinalSabaina RazaОценок пока нет
- Dislocation Shoulder GoodДокумент7 страницDislocation Shoulder GoodZahiera NajibОценок пока нет
- Cools 2008 Screening The Athletes Shoulder ForДокумент9 страницCools 2008 Screening The Athletes Shoulder ForLucyFloresОценок пока нет
- Shoulder Dislocation Background: Shoulder Dislocations Traumatic InjuryДокумент7 страницShoulder Dislocation Background: Shoulder Dislocations Traumatic Injuryanastasiaanggita_265Оценок пока нет
- Rehabilitation For Shoulder Instability: A Jaggi, S LambertДокумент9 страницRehabilitation For Shoulder Instability: A Jaggi, S LambertMarcelo BenitezОценок пока нет
- June1997 CC WilkДокумент10 страницJune1997 CC WilkwesleythompsonОценок пока нет
- Case Report Rehabilitation Program in Patient With Ankle FractureДокумент26 страницCase Report Rehabilitation Program in Patient With Ankle FractureNatalia LoredanaОценок пока нет
- Clinical Tests of The Shoulder: Accuracy and Extension Using Dynamic UltrasoundДокумент9 страницClinical Tests of The Shoulder: Accuracy and Extension Using Dynamic UltrasoundMohammad Al AbdullaОценок пока нет
- Acute Traumatic Posterior Shoulder Dislocation PDFДокумент8 страницAcute Traumatic Posterior Shoulder Dislocation PDFMuhammad Pringgo ArifiantoОценок пока нет
- Shoulder Injuries in The Throwing Athlete: J Bone Joint Surg AmДокумент14 страницShoulder Injuries in The Throwing Athlete: J Bone Joint Surg AmRosaneLacerdaОценок пока нет
- Principles of Spine Trauma and Spinal Deformities PDFДокумент34 страницыPrinciples of Spine Trauma and Spinal Deformities PDFVirlan Vasile CatalinОценок пока нет
- Physical Therapy Management in Shoulder InstabilitiesДокумент7 страницPhysical Therapy Management in Shoulder InstabilitiesYeshvi sОценок пока нет
- Glenoid LabrumДокумент26 страницGlenoid LabrumluizamgoОценок пока нет
- Spinal InstabilityДокумент6 страницSpinal InstabilityMichael PrayogoОценок пока нет
- Anatomy, Pathomechanics and Pathophysiology of Lateral Ankle InstabilityДокумент12 страницAnatomy, Pathomechanics and Pathophysiology of Lateral Ankle InstabilityVinay KumarОценок пока нет
- William C. Cottrell, MD AbstractДокумент4 страницыWilliam C. Cottrell, MD AbstractmalaОценок пока нет
- Approach To The Patient With Muscle Weakness - UpToDateДокумент12 страницApproach To The Patient With Muscle Weakness - UpToDatePatriciaОценок пока нет
- Case Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureДокумент26 страницCase Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureNatalia LoredanaОценок пока нет
- Aaos 2002Документ120 страницAaos 2002Yusufa ArdyОценок пока нет
- Eck 2004Документ13 страницEck 2004Hari25885Оценок пока нет
- Physical Examination of The ElbowДокумент9 страницPhysical Examination of The ElbowpuchioОценок пока нет
- Current Concepts in Shoulder Examination of The Overhead Athlete PDFДокумент25 страницCurrent Concepts in Shoulder Examination of The Overhead Athlete PDFElaine CspОценок пока нет
- Elbow Rehabilitation - SpringerLinkДокумент35 страницElbow Rehabilitation - SpringerLinkasdfОценок пока нет
- Clinical Tests For Evaluation of Motor Function of The ShoulderДокумент10 страницClinical Tests For Evaluation of Motor Function of The ShoulderNader AlkhateebОценок пока нет
- Case Report Rehabilitation Program in A Patient With Tibial Condyle FractureДокумент26 страницCase Report Rehabilitation Program in A Patient With Tibial Condyle FractureNatalia LoredanaОценок пока нет
- 6002 Spine: American Academy of Orthopaedic SurgeonДокумент52 страницы6002 Spine: American Academy of Orthopaedic SurgeonHéctor Pando SánchezОценок пока нет
- Aaos 2019Документ283 страницыAaos 2019alealer2708Оценок пока нет
- Sindrome Impacto Acta Orto Bras 2011 InglДокумент5 страницSindrome Impacto Acta Orto Bras 2011 InglMichele GonçalvesОценок пока нет
- The Painful Shoulder: Part I. Clinical Evaluation - AAFPДокумент18 страницThe Painful Shoulder: Part I. Clinical Evaluation - AAFPMelvin Florens Tania GongaОценок пока нет
- A Modeling Approach To Compute Modification of Net Joint Forces Caused by Coping Movements in Obstetric Brachial Plexus PalsyДокумент9 страницA Modeling Approach To Compute Modification of Net Joint Forces Caused by Coping Movements in Obstetric Brachial Plexus PalsychikaОценок пока нет
- 0 2010 Rehabilitation of Shoulder Impingement Syndrome AnДокумент11 страниц0 2010 Rehabilitation of Shoulder Impingement Syndrome AnTheologos PardalidisОценок пока нет
- Throwing RehabДокумент16 страницThrowing RehabSean GlynnОценок пока нет
- Case Report Rehabilitation Program in A Patient With Left Intertrochanteric Femoral FractureДокумент26 страницCase Report Rehabilitation Program in A Patient With Left Intertrochanteric Femoral FractureNatalia LoredanaОценок пока нет
- Shoulder Injuries and SportДокумент12 страницShoulder Injuries and SportSurgicalgownОценок пока нет
- Spine InjuriesДокумент58 страницSpine InjuriesVinwin777Оценок пока нет
- Posterior Cruciate Ligament InjuriesДокумент26 страницPosterior Cruciate Ligament InjuriesGopi KrishnanОценок пока нет
- Low Back Pain: Anwar SuhaimiДокумент24 страницыLow Back Pain: Anwar SuhaimiAfonso RochaОценок пока нет
- The Lumbar Spine: Understanding The Science Behind Both Movement and Dysfunction by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMSДокумент9 страницThe Lumbar Spine: Understanding The Science Behind Both Movement and Dysfunction by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMSChrisGellertОценок пока нет
- Elbow Arthritis and Removal of Loose Bodies and SpursДокумент11 страницElbow Arthritis and Removal of Loose Bodies and SpurspuchioОценок пока нет
- 2 Current Concepts in The Rehabilitation 1144851241Документ16 страниц2 Current Concepts in The Rehabilitation 1144851241César ArveláezОценок пока нет
- Imaging of Shoulder Pain in Overhead Throwing AthletesДокумент8 страницImaging of Shoulder Pain in Overhead Throwing AthletesLívia PogettiОценок пока нет
- The Painful Shoulder - Part I. Clinical Evaluation PDFДокумент17 страницThe Painful Shoulder - Part I. Clinical Evaluation PDFOscar FrizziОценок пока нет
- 2013 Glenohumeral Motion Deficits, Friend or FoeДокумент17 страниц2013 Glenohumeral Motion Deficits, Friend or FoeIsrael Matías Chandia RamírezОценок пока нет
- Assignment 14a Final PaperДокумент11 страницAssignment 14a Final Paperapi-665233380Оценок пока нет
- Upper Extremity Weightlifting Injuries: Diagnosis and ManagementДокумент6 страницUpper Extremity Weightlifting Injuries: Diagnosis and ManagementsinduОценок пока нет
- Методичка The shoulder and upper armДокумент23 страницыМетодичка The shoulder and upper armzekoОценок пока нет
- Isolated Medial Collateral Ligament Injuries in The KneeДокумент6 страницIsolated Medial Collateral Ligament Injuries in The KneekenthepaОценок пока нет
- Anterior Shoulder InstabilityДокумент19 страницAnterior Shoulder InstabilitySiti Nur JannahОценок пока нет
- Acromioclavicular Joint Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandAcromioclavicular Joint Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- A Simple Guide to Shoulder Muscle Sprain, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Shoulder Muscle Sprain, Diagnosis, Treatment and Related ConditionsОценок пока нет
- The Body: Drawing MangaДокумент17 страницThe Body: Drawing MangaMichaelhmОценок пока нет
- An Overview of Facilitated Stretching - Robert E. McAtee - A-9Документ9 страницAn Overview of Facilitated Stretching - Robert E. McAtee - A-9Tito AlhoОценок пока нет
- MRMДокумент39 страницMRMZafirnur Amrin JasmanОценок пока нет
- Shoulder ComplexДокумент55 страницShoulder ComplexKim VillalobosОценок пока нет
- Muscle QuizДокумент10 страницMuscle QuizFitzgerald PachecoОценок пока нет
- Physical Therapy Protocols For Conditions of Shoulder RegionДокумент111 страницPhysical Therapy Protocols For Conditions of Shoulder RegionPieng Napa100% (1)
- Shoulder MuscleДокумент52 страницыShoulder Muscleshahirah770% (1)
- Gregory I. Bain, Eiji Itoi, Giovanni Di Giacomo, Hiroyuki Sugaya Eds. Normal and Pathological Anatomy of The ShoulderДокумент410 страницGregory I. Bain, Eiji Itoi, Giovanni Di Giacomo, Hiroyuki Sugaya Eds. Normal and Pathological Anatomy of The ShoulderNikolaos Anastasopoulos100% (3)
- Brachial Plexus PowerpointДокумент37 страницBrachial Plexus PowerpointMuhammad Naqiuddin JalaluddinОценок пока нет
- History ExaminationДокумент18 страницHistory ExaminationMohammed FaragОценок пока нет
- Additional Abstracts: The Bear-Hug Test: A New and Sensitive Test For Diagnosing A Subscapularis TearДокумент9 страницAdditional Abstracts: The Bear-Hug Test: A New and Sensitive Test For Diagnosing A Subscapularis Tearo7113Оценок пока нет
- SinulДокумент86 страницSinulCucos NataliaОценок пока нет
- Effect of Barbell Weight On The Structure of The Flat Bench PressДокумент17 страницEffect of Barbell Weight On The Structure of The Flat Bench PressEijunОценок пока нет
- Massage Therapy For Bruxism, TMJ SyndromeДокумент39 страницMassage Therapy For Bruxism, TMJ SyndromeAdam Kesher100% (1)
- Proximal Humerus - Approach - Deltopectoral Approach To The Proximal Humerus - AO Surgery ReferenceДокумент6 страницProximal Humerus - Approach - Deltopectoral Approach To The Proximal Humerus - AO Surgery ReferenceRabin Das0% (1)
- Bench Press SyndromeДокумент4 страницыBench Press SyndromeAbdallah Maroun NajemОценок пока нет
- Girevoy Sport and Athlete Preparation PDFДокумент94 страницыGirevoy Sport and Athlete Preparation PDFLisandro CacciatoreОценок пока нет
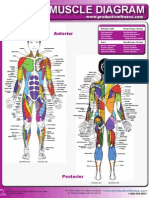
- Female Muscle DiagramДокумент1 страницаFemale Muscle DiagrammakukikiОценок пока нет
- Girevoy Sport and Athlete Preparation 1 3Документ92 страницыGirevoy Sport and Athlete Preparation 1 3dfkr236100% (3)
- D1. Neurologic ExaminationДокумент33 страницыD1. Neurologic ExaminationpancseszОценок пока нет
- Drawing ChildrenДокумент94 страницыDrawing Childrenaleah100% (2)