Вам также может понравиться
- Price List Indian Hill MS and HS 2021Документ1 страницаPrice List Indian Hill MS and HS 2021valuatОценок пока нет
- Quality Enrichment Program For Intellectually Gifted ChildrenДокумент4 страницыQuality Enrichment Program For Intellectually Gifted ChildrenvaluatОценок пока нет
- 3rd Grade Nonverbal Practice ActivitiesДокумент8 страниц3rd Grade Nonverbal Practice ActivitiesvaluatОценок пока нет
- INDIAN HILL HS WELCOME LETTER 2021 W URLДокумент1 страницаINDIAN HILL HS WELCOME LETTER 2021 W URLvaluatОценок пока нет
- Jeffrey Epstein39s Little Black Book Unredacted PDFДокумент95 страницJeffrey Epstein39s Little Black Book Unredacted PDFasdasdasd100% (2)
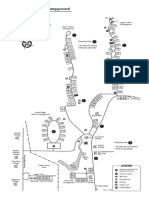
- Tar Hollow State Park CampgroundДокумент1 страницаTar Hollow State Park CampgroundvaluatОценок пока нет
- Fully Automated Echocardiogram Interpretation in Clinical PracticeДокумент13 страницFully Automated Echocardiogram Interpretation in Clinical PracticevaluatОценок пока нет
- Winter/Spring Term Class List: The Super Saturday ProgramДокумент11 страницWinter/Spring Term Class List: The Super Saturday ProgramvaluatОценок пока нет
- Bimcom: User ManualДокумент33 страницыBimcom: User ManualvaluatОценок пока нет
- Working Memory Index: Measures Concentration, Recall, and SequencingДокумент1 страницаWorking Memory Index: Measures Concentration, Recall, and SequencingvaluatОценок пока нет
- Nutrients: Covid-19 Confinement and Changes of Adolescent's Dietary Trends in Italy, Spain, Chile, Colombia and BrazilДокумент18 страницNutrients: Covid-19 Confinement and Changes of Adolescent's Dietary Trends in Italy, Spain, Chile, Colombia and BrazilpatriciaОценок пока нет
- TCF TakeOut LibertyCenter 0816Документ10 страницTCF TakeOut LibertyCenter 0816Cristiana AmarieiОценок пока нет
- The T-Cell ArmyДокумент14 страницThe T-Cell ArmyvaluatОценок пока нет
- SBG6950-7400AC2 User GuideДокумент63 страницыSBG6950-7400AC2 User GuidevaluatОценок пока нет
- WISC IV Five FactorДокумент10 страницWISC IV Five FactorvaluatОценок пока нет
- Ravens SPM Answer SheetДокумент1 страницаRavens SPM Answer SheetvaluatОценок пока нет
- Ead For j-2Документ44 страницыEad For j-2valuatОценок пока нет
- Pub Pedi AtriaДокумент5 страницPub Pedi AtriavaluatОценок пока нет
- WISC IV Handout PDFДокумент121 страницаWISC IV Handout PDFvaluat100% (1)
- WISC-IV Technical Report #1 Theoretical Model and Test BlueprintДокумент7 страницWISC-IV Technical Report #1 Theoretical Model and Test Blueprintعبد الحميد المزينОценок пока нет
- The Gatekeeper and The Wizard A Fairy Tale BMJДокумент3 страницыThe Gatekeeper and The Wizard A Fairy Tale BMJElenaSerranoFdezОценок пока нет
- 10 Things The Most Successful People Do Every Day - TimeДокумент10 страниц10 Things The Most Successful People Do Every Day - Timevaluat100% (1)
- Breast Cancer Screening GuidelinesДокумент4 страницыBreast Cancer Screening GuidelinesvaluatОценок пока нет
- 57 TH Short Course ScheduleДокумент10 страниц57 TH Short Course SchedulevaluatОценок пока нет
- 2018 NGS FlyerДокумент2 страницы2018 NGS FlyervaluatОценок пока нет
- TuringSpecialIssue (Nature2012) PDFДокумент2 страницыTuringSpecialIssue (Nature2012) PDFvaluatОценок пока нет
- Combined Programs Pediatrics-Genetics PDFДокумент3 страницыCombined Programs Pediatrics-Genetics PDFvaluatОценок пока нет
- Ada 420330Документ100 страницAda 420330valuatОценок пока нет
- Bls ProviderДокумент2 страницыBls ProvidermonickamsОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Noreen CVДокумент3 страницыNoreen CVpeace doveОценок пока нет
- Book On Bussiness Statisitics!!!Документ565 страницBook On Bussiness Statisitics!!!DrRam Singh Kamboj0% (1)
- GE PC Course SyllabusДокумент9 страницGE PC Course SyllabusAine CebedoОценок пока нет
- Strategic Plan Revised Version HcdaДокумент74 страницыStrategic Plan Revised Version Hcdaoloograce100% (1)
- (3-Macmillan) Analysing Qualitative DataДокумент23 страницы(3-Macmillan) Analysing Qualitative DataNgọc NgânОценок пока нет
- Research Paper - Blue Moon Group PDFДокумент62 страницыResearch Paper - Blue Moon Group PDFNguyễn Võ Hoàng AnОценок пока нет
- What Do Acute Stroke Physiotherapists Do To Treat Postural Control and MobilityДокумент5 страницWhat Do Acute Stroke Physiotherapists Do To Treat Postural Control and MobilityAugusto ManoelОценок пока нет
- ShortageofaccountingphdsДокумент10 страницShortageofaccountingphdsRizwan M KhanОценок пока нет
- G11 Statistics and Probability Q3 M1Документ10 страницG11 Statistics and Probability Q3 M1Queen Alexza PrandasОценок пока нет
- Customer Relationship Management-HeroДокумент9 страницCustomer Relationship Management-Heromohammed khayyumОценок пока нет
- When Richard Schechner First Coined The TermДокумент2 страницыWhen Richard Schechner First Coined The TermDanah MnlsuОценок пока нет
- Abstract BookДокумент241 страницаAbstract BookMuhammad AsaduzzamanОценок пока нет
- Karachi University Business School (Kubs)Документ6 страницKarachi University Business School (Kubs)Arsalan Mushtaq NCPОценок пока нет
- Polymorphism in CocrystalsДокумент15 страницPolymorphism in CocrystalsBenjamín Marc Ridgway de SassouОценок пока нет
- ISO Audit ChecklistДокумент21 страницаISO Audit Checklistghostghost12380% (5)
- Biosimilarity The FDA Perspective (Sarfaraz K. Niazi) 2019Документ436 страницBiosimilarity The FDA Perspective (Sarfaraz K. Niazi) 2019buuОценок пока нет
- Data Science QuestionsДокумент16 страницData Science QuestionsRohan ChandrashekarОценок пока нет
- MGNREGAДокумент50 страницMGNREGASameesh Khunger100% (1)
- Nuraini Safitri: Bachelor of Urban and Regional PlanningДокумент2 страницыNuraini Safitri: Bachelor of Urban and Regional PlanningRhani Jojoba DholphinОценок пока нет
- MCS Guide To The Datasets 022014 PDFДокумент107 страницMCS Guide To The Datasets 022014 PDFjhoanОценок пока нет
- Worklog 5761 SyncДокумент14 страницWorklog 5761 Synctuanhai1989Оценок пока нет
- Module 3 Principles of High Quality AssessmentДокумент9 страницModule 3 Principles of High Quality AssessmentRycel JucoОценок пока нет
- Transportation Engineering Thesis Topics PhilippinesДокумент4 страницыTransportation Engineering Thesis Topics Philippineshcivczwff100% (1)
- Thesis Report of Aqsa Bashir 7505Документ23 страницыThesis Report of Aqsa Bashir 7505Shehar BanoОценок пока нет
- Durnova & Zittoun, 2013Документ10 страницDurnova & Zittoun, 2013Pantelis TsavalasОценок пока нет
- Tourist LoyaltyДокумент19 страницTourist LoyaltyAditya HendraОценок пока нет
- A BSC Framework For Air Cargo Terminal DesignДокумент10 страницA BSC Framework For Air Cargo Terminal DesignPerry WengОценок пока нет
- Social Structures in Learning Filipino Pedagogy of Preservice Teachers: An Innovative StrategiesДокумент7 страницSocial Structures in Learning Filipino Pedagogy of Preservice Teachers: An Innovative StrategiesPsychology and Education: A Multidisciplinary JournalОценок пока нет
- Massey University Low Decile School Research Paper PDFДокумент58 страницMassey University Low Decile School Research Paper PDFSaranyaОценок пока нет
- MBA ProjectДокумент94 страницыMBA ProjectAnand Swami100% (1)