Вам также может понравиться
- Payroll Management in Simhapuri Hospitals: 1.2 Industry ProfileДокумент30 страницPayroll Management in Simhapuri Hospitals: 1.2 Industry ProfilebhuvanaОценок пока нет
- Nzs 4121 2001 PDFДокумент130 страницNzs 4121 2001 PDFpaulОценок пока нет
- As 1428.2-1992 Design For Access and Mobility Enhanced and Additional Requirements - Buildings and FacilitiesДокумент7 страницAs 1428.2-1992 Design For Access and Mobility Enhanced and Additional Requirements - Buildings and FacilitiesSAI Global - APAC0% (4)
- The National Building Code of India (NBC), A Comprehensive Building Code, Is AДокумент10 страницThe National Building Code of India (NBC), A Comprehensive Building Code, Is AShivani SisodiaОценок пока нет
- Accessibility To Lifts For Persons, Including Persons With DisabilityДокумент26 страницAccessibility To Lifts For Persons, Including Persons With DisabilityCostin Rusen100% (2)
- Chapter 1-3Документ55 страницChapter 1-3Mark Ryan Nagales0% (1)
- 3 Star Hotel Lit StudyДокумент68 страниц3 Star Hotel Lit Studyaruna100% (2)
- Thesis ShereeДокумент78 страницThesis ShereeSheree Nichole GuillerganОценок пока нет
- Le CorbusierДокумент14 страницLe CorbusierResende Architecture WorkОценок пока нет
- Health Care Service IndustryДокумент15 страницHealth Care Service Industryranasarkar123Оценок пока нет
- Hospital Administration 2Документ12 страницHospital Administration 2Mian Muhammad Rashid100% (1)
- Introduction To HospitalsДокумент26 страницIntroduction To Hospitalssurbhi aggarwalОценок пока нет
- Act 1 Manamparan Hosny M.Документ8 страницAct 1 Manamparan Hosny M.Gizelle Mae Pasiol-Macayan100% (2)
- Hospitals and Community Benefit: New Demands, New ApproachesОт EverandHospitals and Community Benefit: New Demands, New ApproachesОценок пока нет
- Medical Social WorkДокумент23 страницыMedical Social WorkHomayoon Nowrozi100% (1)
- Transferring of PatientДокумент11 страницTransferring of Patientyuuna yuunaОценок пока нет
- Planning and Organization of Hospital: Mr. Rakesh Patidar JCN, BhanduДокумент62 страницыPlanning and Organization of Hospital: Mr. Rakesh Patidar JCN, BhanduRakersh Patidar60% (5)
- Hospital FinanceДокумент54 страницыHospital FinancePadmanabha Narayan100% (3)
- The Role of Nursing Homes in ACOsДокумент4 страницыThe Role of Nursing Homes in ACOsrjg427Оценок пока нет
- Physical EnvironmentДокумент16 страницPhysical Environmentangel panchal100% (1)
- Unit 4222-316Документ3 страницыUnit 4222-316Akular AyramОценок пока нет
- Major Stakeholders in Health Care SystemДокумент5 страницMajor Stakeholders in Health Care SystemANITTA S100% (1)
- Hospital Planing and OrganizationДокумент15 страницHospital Planing and OrganizationUdaya SreeОценок пока нет
- Prelim To Finals RT 203 1Документ71 страницаPrelim To Finals RT 203 1Leopardas, Lynn Clemard C.100% (1)
- IPHS Guidelines For District Hospitals (101 To 500 Bedded) PDFДокумент124 страницыIPHS Guidelines For District Hospitals (101 To 500 Bedded) PDFSatish Vaidya67% (3)
- WeeFIM Score Sheet Brain InjuryДокумент3 страницыWeeFIM Score Sheet Brain InjuryDinang Jung100% (2)
- Transforming Healthcare: Healing You, Me, and Our Broken Disease-Care SystemОт EverandTransforming Healthcare: Healing You, Me, and Our Broken Disease-Care SystemОценок пока нет
- Hospital AdministrationДокумент7 страницHospital Administrationburhan shahОценок пока нет
- RE200 - Research Work 2 Hospital Design - Oliveros - Arc42Документ34 страницыRE200 - Research Work 2 Hospital Design - Oliveros - Arc42John Patrick OliverosОценок пока нет
- HOSPI Hospital and Its OrganizationДокумент31 страницаHOSPI Hospital and Its OrganizationAlecxir PharmacyОценок пока нет
- 050d40a6d214cb - Clinical & Hospital Pharmacy - Chapter 1Документ6 страниц050d40a6d214cb - Clinical & Hospital Pharmacy - Chapter 1Absar Ahmad DarОценок пока нет
- Chandana Project 2Документ15 страницChandana Project 2bhuvanaОценок пока нет
- Basic Concept of Hospital and HealthДокумент15 страницBasic Concept of Hospital and Healthmanik ghoshОценок пока нет
- Compare - Contrast Medical CentersДокумент3 страницыCompare - Contrast Medical Centersapi-644961102Оценок пока нет
- Introduction To HospitalДокумент18 страницIntroduction To HospitalSamir SaiyadОценок пока нет
- 1Документ158 страниц1Sulieman Khalifa ArafaОценок пока нет
- Unbundling The HospitalДокумент5 страницUnbundling The Hospitalcrb202Оценок пока нет
- The Value of Healthcare AdministrationДокумент3 страницыThe Value of Healthcare AdministrationKrizzella ShainaОценок пока нет
- Hospital Administration: By: Mrs. Anupama Oka M.SC (N)Документ19 страницHospital Administration: By: Mrs. Anupama Oka M.SC (N)Shreyas OkaОценок пока нет
- VenkateshДокумент21 страницаVenkateshNarendar MОценок пока нет
- Hospital Pharmacy The Hospitals and Its OrganizationДокумент18 страницHospital Pharmacy The Hospitals and Its Organizationranemabdo22Оценок пока нет
- Rittik Shee Classification of HospitalsДокумент10 страницRittik Shee Classification of HospitalsR SheeОценок пока нет
- Pharmacy Practice IntroductionДокумент20 страницPharmacy Practice IntroductionboyapallymeghanaОценок пока нет
- Charitable Organizations Were The Main Providers of Subsidized HealthcareДокумент6 страницCharitable Organizations Were The Main Providers of Subsidized HealthcareGautam MahilaryОценок пока нет
- Role of Health InsuranceДокумент1 страницаRole of Health InsurancePijus GhoshОценок пока нет
- Health Care USA Chapter 4Документ53 страницыHealth Care USA Chapter 4David TurnerОценок пока нет
- Hospital Theory 1 1Документ6 страницHospital Theory 1 1Anoop Gupta054Оценок пока нет
- General: 1.) Identify The Four Hospital Functions and Give A Brief DescriptionДокумент3 страницыGeneral: 1.) Identify The Four Hospital Functions and Give A Brief DescriptionHazelОценок пока нет
- FORMATДокумент7 страницFORMATaarthyОценок пока нет
- Public HospitalДокумент6 страницPublic HospitalALWAHIDAОценок пока нет
- Week 1-3 Topics, NotesДокумент6 страницWeek 1-3 Topics, NotesChunnie JakosalemОценок пока нет
- Hospital Pharmacy Notes Weeks 1 4Документ17 страницHospital Pharmacy Notes Weeks 1 4Chunnie JakosalemОценок пока нет
- HospitalsДокумент16 страницHospitalsgemergencycareОценок пока нет
- Major Stakeholders Satyajit MamДокумент11 страницMajor Stakeholders Satyajit MamAnchal thakurОценок пока нет
- 3.2 Major Stake HoldersДокумент51 страница3.2 Major Stake HoldersSwati SharmaОценок пока нет
- The Role of Architecture in Promoting Healing Environments in The Design of Small, Rural HospitalsДокумент6 страницThe Role of Architecture in Promoting Healing Environments in The Design of Small, Rural Hospitalsellica123Оценок пока нет
- Study On Floor Mangement FinalДокумент65 страницStudy On Floor Mangement FinalBrok GamingОценок пока нет
- INI DIAAAA t60708Документ89 страницINI DIAAAA t60708Debby Adhila ShanahanОценок пока нет
- Presentation1 Copy 2Документ5 страницPresentation1 Copy 2Eva Bardaje-AgasОценок пока нет
- MekdishaaaaaДокумент12 страницMekdishaaaaatewodros bayisaОценок пока нет
- HospitalsДокумент29 страницHospitalsAkash PawarОценок пока нет
- 09 Chapter 1Документ45 страниц09 Chapter 1Madhusudan MОценок пока нет
- Branding of Hospitals Through Tangible Factors by Selected HospitalsДокумент12 страницBranding of Hospitals Through Tangible Factors by Selected HospitalsMeghaОценок пока нет
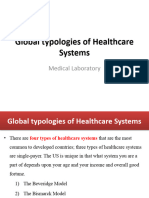
- Global Typologies of Healthcare SystemsДокумент12 страницGlobal Typologies of Healthcare SystemstewodrosbayisaОценок пока нет
- Continuous Improvment Quality Improvment in Health Care - Case 1Документ40 страницContinuous Improvment Quality Improvment in Health Care - Case 1Linda Vono100% (1)
- D4Документ28 страницD4Ciara AnneОценок пока нет
- Ser Unit 5Документ118 страницSer Unit 5Aneesh DominicОценок пока нет
- Summer Internship ReportДокумент55 страницSummer Internship ReportModi Em100% (3)
- Synopsis - Rohan Birajdar.5thYRДокумент10 страницSynopsis - Rohan Birajdar.5thYRRohan BirajdarОценок пока нет
- Selling Our Souls: The Commodification of Hospital Care in the United StatesОт EverandSelling Our Souls: The Commodification of Hospital Care in the United StatesОценок пока нет
- Architecture Work Chart by AnushakanchiДокумент5 страницArchitecture Work Chart by AnushakanchianushakanchiОценок пока нет
- Anusha Kanchi - Portfolio - PDF (SmallДокумент23 страницыAnusha Kanchi - Portfolio - PDF (SmallanushakanchiОценок пока нет
- Thanks SCRDДокумент1 страницаThanks SCRDanushakanchiОценок пока нет
- 1jbuh Io Iomijkjhi Ynmkyg, MuДокумент1 страница1jbuh Io Iomijkjhi Ynmkyg, MuanushakanchiОценок пока нет
- Work Chart Ipoioii Iyiuny, Uyuinyyliylinylyluluii7y7yДокумент2 страницыWork Chart Ipoioii Iyiuny, Uyuinyyliylinylyluluii7y7yanushakanchiОценок пока нет
- 2huhhh Oijo Ij Ioji Ojijijiji Ji oДокумент1 страница2huhhh Oijo Ij Ioji Ojijijiji Ji oanushakanchiОценок пока нет
- Why Ancient Toy Makers of Karnataka Are Being Forced To Give Up Their CraftДокумент44 страницыWhy Ancient Toy Makers of Karnataka Are Being Forced To Give Up Their CraftanushakanchiОценок пока нет
- Shivara SiteeДокумент1 страницаShivara SiteeanushakanchiОценок пока нет
- WWOOF India Organics PVT LTD: Registration Number U01403UR 2010 PTC 033280Документ131 страницаWWOOF India Organics PVT LTD: Registration Number U01403UR 2010 PTC 033280anushakanchiОценок пока нет
- SДокумент1 страницаSanushakanchiОценок пока нет
- HahahahaДокумент1 страницаHahahahaanushakanchiОценок пока нет
- History of Hospitals.11155632Документ10 страницHistory of Hospitals.11155632anushakanchiОценок пока нет
- Arjo BedДокумент6 страницArjo BedscoobysmackОценок пока нет
- CITY STAR Newspaper January 2018Документ11 страницCITY STAR Newspaper January 2018city star newspaperОценок пока нет
- Application of The Functional, Expressive and Aesthetic Consumer Needs Model Assessing The Clothing Needs of Adolescent Girls With DisabilitiesДокумент10 страницApplication of The Functional, Expressive and Aesthetic Consumer Needs Model Assessing The Clothing Needs of Adolescent Girls With DisabilitiesAsish DasОценок пока нет
- Infrared Non-Contact Head Sensor, For Control of Wheelchair MovementsДокумент5 страницInfrared Non-Contact Head Sensor, For Control of Wheelchair MovementsJainul PatelОценок пока нет
- Reserve Is No Place For A Wheelchair Challenges To Consider During Wheelchair Provision Intended For Use in First Nations CommunityДокумент9 страницReserve Is No Place For A Wheelchair Challenges To Consider During Wheelchair Provision Intended For Use in First Nations CommunityJulieAdamBabinОценок пока нет
- Vos Workbook EnglishДокумент19 страницVos Workbook EnglishErling MountОценок пока нет
- Braden ScaleДокумент3 страницыBraden Scalejackson wong100% (1)
- Wudu Workstation Design For Elderly and DisabledДокумент11 страницWudu Workstation Design For Elderly and DisabledHang AyyaОценок пока нет
- Unit 5: PhysiotherapyДокумент9 страницUnit 5: PhysiotherapyBial MediaОценок пока нет
- Hamilton - Lme UppДокумент18 страницHamilton - Lme UppSergio Navarrete VidalОценок пока нет
- RRLLLLLLLLLLДокумент3 страницыRRLLLLLLLLLLErryl Justine AdvinculaОценок пока нет
- Functional Status Score For The Intensive Care Unit (FSS-ICU) General Guidelines For ScoringДокумент7 страницFunctional Status Score For The Intensive Care Unit (FSS-ICU) General Guidelines For ScoringBennisonОценок пока нет
- Chapter - 2Документ30 страницChapter - 2Rgirish 1Оценок пока нет
- Task 2 Meet Personal NeedsДокумент3 страницыTask 2 Meet Personal Needsdev kumarОценок пока нет
- Research PPR Electric ScooterДокумент4 страницыResearch PPR Electric ScooterRachit GuptaОценок пока нет
- Annex A - Technical SpecificationsДокумент21 страницаAnnex A - Technical SpecificationsSajjadul MawlaОценок пока нет
- Medicotech Thera-Trainer Catalogue Home EditionДокумент33 страницыMedicotech Thera-Trainer Catalogue Home Editionweb-studioОценок пока нет
- Activity Daily Living (ADL)Документ36 страницActivity Daily Living (ADL)Akmal IzaanОценок пока нет
- Mobility Aids Vehicles BizHouse - UkДокумент3 страницыMobility Aids Vehicles BizHouse - UkAlex BekeОценок пока нет
- Societies: Accessibility in Inclusive Tourism? Hotels Distributed Through Online ChannelsДокумент12 страницSocieties: Accessibility in Inclusive Tourism? Hotels Distributed Through Online ChannelsNurul IzzatyОценок пока нет