Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- DeveshДокумент14 страницDeveshAr Aditya SagarОценок пока нет
- Pharmacology of Phenadoxone dN-Morpholino 4:4 Diphenyl: HydrochlorideДокумент17 страницPharmacology of Phenadoxone dN-Morpholino 4:4 Diphenyl: Hydrochlorideisaev201Оценок пока нет
- Questionnnaire 1Документ3 страницыQuestionnnaire 1Franz Sobrejuanite GuillemОценок пока нет
- Adderall-Safer Than AspirinДокумент2 страницыAdderall-Safer Than AspirinChristopher RhudyОценок пока нет
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Документ7 страницScope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Ar Aditya SagarОценок пока нет
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Документ6 страницScope of Work Prime Club Area Rs./Sqft. Total Wood Work Closet (Laminate Finish)Ar Aditya SagarОценок пока нет
- Washroom Washroom 1: GurugramДокумент4 страницыWashroom Washroom 1: GurugramAr Aditya SagarОценок пока нет
- Scope of Work Prime Club Area Rs./Sqft. Total Wood Work: Paint WallpaperДокумент5 страницScope of Work Prime Club Area Rs./Sqft. Total Wood Work: Paint WallpaperAr Aditya SagarОценок пока нет
- Scope of Work: To, MR - Pradeep Tower 16 Flat No-1606 Jaypee Kosmos Sector 134 NoidaДокумент1 страницаScope of Work: To, MR - Pradeep Tower 16 Flat No-1606 Jaypee Kosmos Sector 134 NoidaAr Aditya SagarОценок пока нет
- Laminates-Inner Surface: Virgo, Outer Surface: Greenlam Note - Fittings - Hettich Boards / Ply - Greenply: Carcass, Action Tesa HDHMR: ShutterДокумент1 страницаLaminates-Inner Surface: Virgo, Outer Surface: Greenlam Note - Fittings - Hettich Boards / Ply - Greenply: Carcass, Action Tesa HDHMR: ShutterAr Aditya SagarОценок пока нет
- Payment Plan Stages Amount DateДокумент1 страницаPayment Plan Stages Amount DateAr Aditya SagarОценок пока нет
- Allotment Date: MS152 13/jul/2019 45040486Документ1 страницаAllotment Date: MS152 13/jul/2019 45040486Ar Aditya SagarОценок пока нет
- HubantДокумент3 страницыHubantAr Aditya SagarОценок пока нет
- Scope of Work Prime Club Area Rs./Sqft. Total Wood WorkДокумент5 страницScope of Work Prime Club Area Rs./Sqft. Total Wood WorkAr Aditya SagarОценок пока нет
- Sanfrancesco 150410041419 Conversion Gate01Документ16 страницSanfrancesco 150410041419 Conversion Gate01Ar Aditya SagarОценок пока нет
- Paint Wallpaper: False Ceiling (Pop J.K/ Sakarni)Документ2 страницыPaint Wallpaper: False Ceiling (Pop J.K/ Sakarni)Ar Aditya SagarОценок пока нет
- JM FLorence QuotationДокумент1 страницаJM FLorence QuotationAr Aditya SagarОценок пока нет
- About The Project:: HABITAT CENTRE Is Now Home Not Only ToДокумент34 страницыAbout The Project:: HABITAT CENTRE Is Now Home Not Only ToAr Aditya SagarОценок пока нет
- AnjaliДокумент1 страницаAnjaliAr Aditya SagarОценок пока нет
- Site PlanДокумент1 страницаSite PlanAr Aditya SagarОценок пока нет
- Ground Floor PlanДокумент1 страницаGround Floor PlanAr Aditya SagarОценок пока нет
- College Plan Single LineДокумент1 страницаCollege Plan Single LineAr Aditya SagarОценок пока нет
- Baroque Architecture (Buildings and Architects) : Submitted ByДокумент14 страницBaroque Architecture (Buildings and Architects) : Submitted ByAr Aditya SagarОценок пока нет
- Elevat inДокумент1 страницаElevat inAr Aditya SagarОценок пока нет
- Thesis Submission Check ListДокумент2 страницыThesis Submission Check ListAr Aditya SagarОценок пока нет
- April 2016Документ82 страницыApril 2016Ar Aditya SagarОценок пока нет
- Ent of FeeДокумент1 страницаEnt of FeeAr Aditya SagarОценок пока нет
- Indian Standard Basic Requirements For Hospital Planning: 0. ForewordДокумент2 страницыIndian Standard Basic Requirements For Hospital Planning: 0. ForewordAr Aditya SagarОценок пока нет
- Buddism Architecture: The Architecture of India Then Move TowardsДокумент2 страницыBuddism Architecture: The Architecture of India Then Move TowardsAr Aditya SagarОценок пока нет
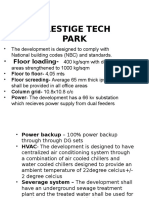
- Prestige Tech Park: - Floor LoadingДокумент9 страницPrestige Tech Park: - Floor LoadingAr Aditya SagarОценок пока нет
- Area Requirement1Документ2 страницыArea Requirement1Ar Aditya SagarОценок пока нет
- Requirments Commercial ComplexДокумент2 страницыRequirments Commercial ComplexAr Aditya SagarОценок пока нет
- 1 Labor and Delivery ProcessДокумент13 страниц1 Labor and Delivery ProcessBardiaga JmayОценок пока нет
- Acute Febrile Illnesses: Solomon Bekele Sirak Melkeneh Sonia Worku Fri. May 15, 2014Документ124 страницыAcute Febrile Illnesses: Solomon Bekele Sirak Melkeneh Sonia Worku Fri. May 15, 2014ashuОценок пока нет
- Non Kepi Vaccines RevisedДокумент28 страницNon Kepi Vaccines Revisedokwadha simionОценок пока нет
- Adaptive and Innate ImmunityДокумент63 страницыAdaptive and Innate ImmunitySarvesh Patil100% (1)
- Analisis Kesesuaian Penggunaan Antiinfeksi Pada Infeksi Oportunistik Pasien Hiv/Aids Rawat Inap Di Rsup Dr. Sardjito YogyakartaДокумент7 страницAnalisis Kesesuaian Penggunaan Antiinfeksi Pada Infeksi Oportunistik Pasien Hiv/Aids Rawat Inap Di Rsup Dr. Sardjito YogyakartaindahОценок пока нет
- Profmed About ProfmedДокумент2 страницыProfmed About ProfmedJesiel Romero RodotaОценок пока нет
- Nhsbi FormДокумент1 страницаNhsbi FormClark Jayden JacobОценок пока нет
- B Blab 6 Crossmatch SP 05Документ14 страницB Blab 6 Crossmatch SP 05Rutchelle Joyce PugoyОценок пока нет
- Methylene Blue For Refractory Shock in Pediatric PatientsДокумент16 страницMethylene Blue For Refractory Shock in Pediatric Patientsandi rahmatОценок пока нет
- Sialometria ClinicaДокумент4 страницыSialometria ClinicaDr. JharОценок пока нет
- Aloe Vera DoajДокумент8 страницAloe Vera DoajNur AiniОценок пока нет
- @ (White Paper Cut-Off) QUS 0202 FinalДокумент13 страниц@ (White Paper Cut-Off) QUS 0202 FinalHajjab AnasОценок пока нет
- Mouth Sores Pictures, Causes, Types, Symptoms, and TreatmentsДокумент1 страницаMouth Sores Pictures, Causes, Types, Symptoms, and Treatmentslashes everafterОценок пока нет
- Structure of The NailДокумент33 страницыStructure of The NailYen100% (1)
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Документ11 страницScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiОценок пока нет
- 20 OncoДокумент115 страниц20 OncomichelleОценок пока нет
- ExamView - Chapter - 33 PDFДокумент8 страницExamView - Chapter - 33 PDFChizua OkoyeОценок пока нет
- Table 1 Classification and Staging Systems For AKIДокумент1 страницаTable 1 Classification and Staging Systems For AKIAnityo NugrohoОценок пока нет
- Mcqs FinalДокумент4 страницыMcqs FinalJats_Fru_1741Оценок пока нет
- Fundamentals of Nursing: BulletsДокумент27 страницFundamentals of Nursing: BulletsKristian Dave DivaОценок пока нет
- BipolarДокумент6 страницBipolarDoniele DalorОценок пока нет
- Bayabas: Instructions For GuavaДокумент2 страницыBayabas: Instructions For GuavadorothypearlОценок пока нет
- Hallux Valgus PDFДокумент26 страницHallux Valgus PDFDeny EvanderОценок пока нет
- Module 4 - Alcohol AbuseДокумент17 страницModule 4 - Alcohol AbuseMark Johnuel DuavisОценок пока нет
- Ballard Score Calculator: CalculatorsДокумент1 страницаBallard Score Calculator: Calculatorsbazlin syabrinaОценок пока нет
- JDO 50 Non-Extraction Treatment of Pseudo Class III Anterior Cross BiteДокумент17 страницJDO 50 Non-Extraction Treatment of Pseudo Class III Anterior Cross BiteLiying JuОценок пока нет
- CDC 26714 DS1Документ383 страницыCDC 26714 DS1Joyce AngobungОценок пока нет