Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Abnormal VermisДокумент1 страницаAbnormal VermiscalmlandОценок пока нет
- Major Categories of Mimics of VasculitisДокумент1 страницаMajor Categories of Mimics of VasculitisDrHellenОценок пока нет
- Combining Antiplatelet and Anticoagulant Therapy in Cardiovascular Disease - 2020 - AHAДокумент7 страницCombining Antiplatelet and Anticoagulant Therapy in Cardiovascular Disease - 2020 - AHADrHellenОценок пока нет
- Non-Vitamin K Antagonist Oral Anticoagulants in Patients with β-Thalassemia 2023Документ8 страницNon-Vitamin K Antagonist Oral Anticoagulants in Patients with β-Thalassemia 2023DrHellenОценок пока нет
- Brain Tumours (Primary) - NICE Guide 2021Документ69 страницBrain Tumours (Primary) - NICE Guide 2021DrHellenОценок пока нет
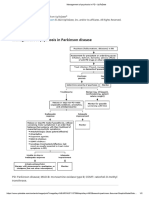
- Management of Psychosis in PDДокумент2 страницыManagement of Psychosis in PDDrHellenОценок пока нет
- An Update On Best Practice of Deep Brain Stimulation in Parkinson's DiseaseДокумент20 страницAn Update On Best Practice of Deep Brain Stimulation in Parkinson's DiseaseDrHellenОценок пока нет
- Handwritten Pattern Recognition For Early Parkinson's Disease Diagnosis - Bernardo2019Документ7 страницHandwritten Pattern Recognition For Early Parkinson's Disease Diagnosis - Bernardo2019DrHellenОценок пока нет
- Boala Binswanger PDFДокумент12 страницBoala Binswanger PDFDrHellenОценок пока нет
- Preventive Strategies For Cognitive Decline and DementiaДокумент13 страницPreventive Strategies For Cognitive Decline and DementiaDrHellenОценок пока нет
- Dementia Prevention, Intervention, and Care - 2020 Report of The Lancet CommissionДокумент35 страницDementia Prevention, Intervention, and Care - 2020 Report of The Lancet CommissionDrHellenОценок пока нет
- 24-06-2020 HMB EnglishДокумент20 страниц24-06-2020 HMB EnglishRakshith GowdaОценок пока нет
- Agricultural Performance Survey of 2021 Wet Season in NigeriaДокумент361 страницаAgricultural Performance Survey of 2021 Wet Season in NigeriaEnemona ShellengОценок пока нет
- Mod 6 Soft Tissue InjuriesДокумент5 страницMod 6 Soft Tissue Injuriesrez1987100% (1)
- Vitamins and Minerals: Nutrient (Vitamins) Needed For Key SourcesДокумент4 страницыVitamins and Minerals: Nutrient (Vitamins) Needed For Key SourcesKevin Carl A. CorpuzОценок пока нет
- Moving The TeethДокумент117 страницMoving The TeethThirunavukkarasu Srinivasan100% (2)
- Week9&10 LEC Clinical Parasitology NEMATODESДокумент18 страницWeek9&10 LEC Clinical Parasitology NEMATODESSamuel ReyesОценок пока нет
- Assessment of The Ear, Nose and ThroatДокумент40 страницAssessment of The Ear, Nose and Throatsnickers_j100% (3)
- Arachnoid Cyst: From Wikipedia, The Free EncyclopediaДокумент11 страницArachnoid Cyst: From Wikipedia, The Free EncyclopediaOsama Bin RizwanОценок пока нет
- KumeДокумент28 страницKumeGrace Clemenia-GrefaldiaОценок пока нет
- Neck Lump HistoryДокумент4 страницыNeck Lump HistoryAlmomnbllah Ahmed100% (1)
- Rabies - WikipediaДокумент22 страницыRabies - WikipediaBruno BusnelloОценок пока нет
- CABERGOLINE Safety2Документ6 страницCABERGOLINE Safety2Kane SmithОценок пока нет
- The Cool Night Breeze Whistled SoftlyДокумент1 страницаThe Cool Night Breeze Whistled SoftlysiddiqpatelОценок пока нет
- Natural Remedies For FibroidsДокумент2 страницыNatural Remedies For Fibroidsafm2026Оценок пока нет
- Wednesday - Session A01 - Arello - Basic Suturing Skills and TechniquesДокумент30 страницWednesday - Session A01 - Arello - Basic Suturing Skills and TechniquesSuresh Thapa ChhetriОценок пока нет
- Risk Management Prelim ReviewerДокумент3 страницыRisk Management Prelim ReviewerCharmaigne BañaresОценок пока нет
- Research Life ScienceДокумент21 страницаResearch Life ScienceKeyth Abegail RendonОценок пока нет
- Chapter 6. The Circulatory System: Short QuestionsДокумент31 страницаChapter 6. The Circulatory System: Short QuestionsParardha DharОценок пока нет
- Function Human HeartДокумент13 страницFunction Human Heartshyam_inkОценок пока нет
- History of NeuroscienceДокумент17 страницHistory of NeurosciencerazorviperОценок пока нет
- 3 Minute German Die KörperteileДокумент11 страниц3 Minute German Die KörperteileBahar TukanovaОценок пока нет
- Top Homeopathic Remedies For ColdsДокумент2 страницыTop Homeopathic Remedies For ColdsAkash kumarОценок пока нет
- Ielts 5.0 l1 R DoneДокумент14 страницIelts 5.0 l1 R DoneMai TrangОценок пока нет
- Anatomy and Physiology of Oral CavityДокумент15 страницAnatomy and Physiology of Oral Cavity28 manan patelОценок пока нет
- Beginner's Guide To Getting Started With DiscusДокумент18 страницBeginner's Guide To Getting Started With DiscusGary HoustonОценок пока нет
- The HelpДокумент7 страницThe HelpRajipah OsmanОценок пока нет
- Allergy Diagnostic TestingДокумент149 страницAllergy Diagnostic TestingArrow Ou100% (1)
- What Is The Effect of Swallowing Without Chewing Properly? What Happen With The Chewing Gum?Документ15 страницWhat Is The Effect of Swallowing Without Chewing Properly? What Happen With The Chewing Gum?Jorge Enrique Olaya LiévanoОценок пока нет
- CALDOBДокумент2 страницыCALDOBSatyendra Pandey50% (2)