Вам также может понравиться
- Medscape Abdominal HerniasДокумент47 страницMedscape Abdominal HerniasSary OktiviaОценок пока нет
- Hernia AbdominalisДокумент45 страницHernia AbdominalisFAIRUZ RIFANIОценок пока нет
- Nursing Assessment: Patient History, An Infant or A Child May Be Relatively Free From Symptom Until She or He CriesДокумент4 страницыNursing Assessment: Patient History, An Infant or A Child May Be Relatively Free From Symptom Until She or He Criescyrilcarinan100% (1)
- Hernias: Dr. Kosov E.V., Department of Surgery and OSTAДокумент53 страницыHernias: Dr. Kosov E.V., Department of Surgery and OSTAprashant singhОценок пока нет
- HerniaДокумент6 страницHerniaHirya jamalОценок пока нет
- HerniaДокумент48 страницHerniaAb BabyОценок пока нет
- Lapkas Hi 4-6-18Документ41 страницаLapkas Hi 4-6-18kalvinОценок пока нет
- Scrotal HerniaДокумент9 страницScrotal HerniaReymart BolagaoОценок пока нет
- What Is Hernia?: Hernia Occurs When An Organ or Fatty TissueДокумент47 страницWhat Is Hernia?: Hernia Occurs When An Organ or Fatty TissuePhuntsho OngmoОценок пока нет
- Inguinal HerniaДокумент8 страницInguinal HerniaAdreiTheTripleAОценок пока нет
- Hernia: Done by D1 GroupДокумент47 страницHernia: Done by D1 Groupanindyadputri100% (1)
- Deviriligo Notes 12Документ99 страницDeviriligo Notes 12A Fish100% (1)
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Документ46 страницAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarОценок пока нет
- Hernia: DR - Surender Singh DhankharДокумент36 страницHernia: DR - Surender Singh DhankharBharat BhushanОценок пока нет
- HerniaДокумент46 страницHerniaZubairkhan SuraniОценок пока нет
- Inguinal Hernia Written ReportДокумент9 страницInguinal Hernia Written ReportpaulaОценок пока нет
- Hernias (Inguinal and Femoral)Документ37 страницHernias (Inguinal and Femoral)Muwanga faizoОценок пока нет
- HerniaДокумент34 страницыHerniaSisay FentaОценок пока нет
- Hernia RepairДокумент5 страницHernia RepairAgung Choro de ObesОценок пока нет
- Untitled DocumentДокумент4 страницыUntitled DocumentNIVISSA BASULGANОценок пока нет
- HerniaДокумент6 страницHerniaKrizette Ann Cuevo BuanОценок пока нет
- HerniaДокумент9 страницHerniaMohammad Yordan GandaraОценок пока нет
- Hernia Examination OSCE GuideДокумент7 страницHernia Examination OSCE GuideEssa AfridiОценок пока нет
- HerniaДокумент47 страницHerniamalathiОценок пока нет
- Nursing Care Plan For Inguinal Hernia HBДокумент4 страницыNursing Care Plan For Inguinal Hernia HBdheeneshbabu0% (1)
- Indirect Inguinal HerniaДокумент25 страницIndirect Inguinal HerniaSheena JaeОценок пока нет
- Types of Hernia and Its ManagementДокумент80 страницTypes of Hernia and Its ManagementVisaagan Kalaithasan50% (2)
- Answer For Case 1Документ8 страницAnswer For Case 1Chefera AgaОценок пока нет
- HerniaДокумент11 страницHerniaHapsari Wibawani 'winda'100% (1)
- Abdominal HerniaДокумент2 страницыAbdominal HerniaWow WuwОценок пока нет
- Inguinal Hernia: Peritoneum, Resulting in A BulgeДокумент5 страницInguinal Hernia: Peritoneum, Resulting in A BulgeJunathan L. Delgado100% (1)
- GS2 HerniaДокумент13 страницGS2 HerniaMAH pedОценок пока нет
- Lecture Notes On Surgery - Part II - Dr. Yogiram BolisettyДокумент79 страницLecture Notes On Surgery - Part II - Dr. Yogiram Bolisettyjun sianОценок пока нет
- Acute AppendicitisДокумент22 страницыAcute AppendicitisJOY LIMBONGОценок пока нет
- HerniaДокумент10 страницHerniaEly Sakti SihotangОценок пока нет
- Examination of The AbdomenДокумент19 страницExamination of The AbdomenAllen AykayОценок пока нет
- Inguinal and Femoral HerniaДокумент50 страницInguinal and Femoral HerniaFafa NabihaОценок пока нет
- Abdominal Hernia: Jama Patient PageДокумент1 страницаAbdominal Hernia: Jama Patient PageSherly CanceritaОценок пока нет
- Inguinal HerniaДокумент6 страницInguinal HerniaignatiuserikОценок пока нет
- Appendicitis Def - It Is An Inflammation of The AppendixДокумент9 страницAppendicitis Def - It Is An Inflammation of The AppendixSanthu SuОценок пока нет
- Acute Abdomen: DR Teamir Negussie Assistant Professor Dept of SurgeryДокумент69 страницAcute Abdomen: DR Teamir Negussie Assistant Professor Dept of SurgeryteamirОценок пока нет
- Hernia Examination OSCE Guide PDFДокумент8 страницHernia Examination OSCE Guide PDFParsaant SinghОценок пока нет
- Abdominal Hernia: Jama Patient PageДокумент1 страницаAbdominal Hernia: Jama Patient PagebasokkaОценок пока нет
- Abdominal Wall Hernia اسامة السنوسيДокумент38 страницAbdominal Wall Hernia اسامة السنوسيAdel SalehОценок пока нет
- AbdomenДокумент48 страницAbdomenAnne Marjorie Futalan100% (1)
- Appendicitis NotesДокумент15 страницAppendicitis NotesHero MondaresОценок пока нет
- What Is An Abdominal Hernia?Документ5 страницWhat Is An Abdominal Hernia?divyanshuguptaОценок пока нет
- Submitted By:: Balacang, Karen L. N-416 Group A Cluster 2 Mr. Raymund P. Bautista RN MAN Clinical Instructor at TCHДокумент26 страницSubmitted By:: Balacang, Karen L. N-416 Group A Cluster 2 Mr. Raymund P. Bautista RN MAN Clinical Instructor at TCHKim BalacangОценок пока нет
- HerniaДокумент24 страницыHerniaSalman HabeebОценок пока нет
- Appendectomy O.R. Write UpДокумент11 страницAppendectomy O.R. Write UpJessica Christine Datuin GustiloОценок пока нет
- Hernia Scrotalis FIxДокумент56 страницHernia Scrotalis FIxivaniОценок пока нет
- Incarcerated Hernia: Case Studies Sushila Ladumor, MDДокумент11 страницIncarcerated Hernia: Case Studies Sushila Ladumor, MDbeautifulbeastОценок пока нет
- APPENDICITISДокумент37 страницAPPENDICITISjohn paul richard mindanaoОценок пока нет
- Inguinal Hernia: From Wikipedia, The Free EncyclopediaДокумент6 страницInguinal Hernia: From Wikipedia, The Free EncyclopediaSherlyn YeeОценок пока нет
- Acute Raptured Appendicitis - VMCДокумент6 страницAcute Raptured Appendicitis - VMCMicahMananguitОценок пока нет
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsРейтинг: 5 из 5 звезд5/5 (1)
- Hernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsРейтинг: 5 из 5 звезд5/5 (1)
- Splenic Abscess: BackgroundДокумент4 страницыSplenic Abscess: BackgroundRizki KhairОценок пока нет
- Abses HeparДокумент4 страницыAbses HeparRizki KhairОценок пока нет
- Tumor Kantong Empesdu Background: Cholesterol PolypsДокумент3 страницыTumor Kantong Empesdu Background: Cholesterol PolypsRizki KhairОценок пока нет
- Pathophysiology: Lipomas LiposarcomasДокумент3 страницыPathophysiology: Lipomas LiposarcomasRizki KhairОценок пока нет
- Perioperative Medicine Managing Surgical Patients With Medical Problems by Chikwe, Joanna Walther, Axel Jones, PhilipДокумент462 страницыPerioperative Medicine Managing Surgical Patients With Medical Problems by Chikwe, Joanna Walther, Axel Jones, PhilipIbrahim AlmohiniОценок пока нет
- Echocardiographic Evaluation of Patent Foramen Ovale Prior To Device ClosureДокумент12 страницEchocardiographic Evaluation of Patent Foramen Ovale Prior To Device ClosureIris AszalosОценок пока нет
- Inguinal HerniaДокумент4 страницыInguinal HerniaRegine SitchonОценок пока нет
- Honey Lorie D. Simbajon - Brain Injury Part IДокумент7 страницHoney Lorie D. Simbajon - Brain Injury Part IMary Grace SimbajonОценок пока нет
- Oral Surgery 2 FinalsДокумент32 страницыOral Surgery 2 FinalsKen HoiОценок пока нет
- ReferensiДокумент4 страницыReferensiBayuAjiWicaksonoОценок пока нет
- 11-C1 BrowliftДокумент34 страницы11-C1 BrowliftShaun Tan100% (1)
- sureerat sua1,+ผู้จัดการวารสาร,+011วารสารหลอดเลือด+Volume+18+No2 2019 2019ThaiGuideline PDFДокумент24 страницыsureerat sua1,+ผู้จัดการวารสาร,+011วารสารหลอดเลือด+Volume+18+No2 2019 2019ThaiGuideline PDFThitipong NonnoiОценок пока нет
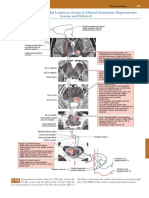
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsДокумент1 страницаPosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezОценок пока нет
- Core Concepts For Local RN ExamsДокумент16 страницCore Concepts For Local RN ExamsChantilly Marie VillarinОценок пока нет
- Intubation ProcedureДокумент5 страницIntubation ProcedurePurwadi SujalmoОценок пока нет
- LAMINECTOMYДокумент22 страницыLAMINECTOMYPatricia CaladoОценок пока нет
- Degenerative ScoliosisДокумент8 страницDegenerative ScoliosisAnonymous 2q4eg3hgEvОценок пока нет
- Nonsurgical Management of Facial Masculinization and Feminization PDFДокумент15 страницNonsurgical Management of Facial Masculinization and Feminization PDFImanuel CristiantoОценок пока нет
- UntitledДокумент2 страницыUntitledAelysa PabloОценок пока нет
- Medical Surgical ReviewerДокумент6 страницMedical Surgical ReviewerCatherine Kaye PerezОценок пока нет
- AEMT - Obstetrics and Pediatrics Exam PracticeДокумент26 страницAEMT - Obstetrics and Pediatrics Exam PracticeEMS DirectorОценок пока нет
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerДокумент6 страницProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanОценок пока нет
- 15 Physio OB - Normal LaborДокумент8 страниц15 Physio OB - Normal LabormaqmmОценок пока нет
- ER & CCU ProtocolДокумент14 страницER & CCU ProtocolatinafansifОценок пока нет
- Test Bank Maternity and Pediatric Nursing 3rd EditionДокумент10 страницTest Bank Maternity and Pediatric Nursing 3rd Editionjeremiahhartfozxmbqayn100% (11)
- Aaron 800 - Eu AARON 900Документ60 страницAaron 800 - Eu AARON 900Carlos Equipamiento M-h M-vОценок пока нет
- PKB XviiДокумент2 страницыPKB XviiRian WaraneyОценок пока нет
- Fabian VentilatorДокумент17 страницFabian VentilatorRohana AnaОценок пока нет
- Begg Stage 2-OrTHO / Orthodontic Courses by Indian Dental AcademyДокумент28 страницBegg Stage 2-OrTHO / Orthodontic Courses by Indian Dental Academyindian dental academyОценок пока нет
- Alison Mann Orthopedic CoursenotesДокумент5 страницAlison Mann Orthopedic CoursenotesaghoescnОценок пока нет
- X & H Plate PDFДокумент2 страницыX & H Plate PDFAngulo HernandezОценок пока нет
- 6 7 Content2Документ2 страницы6 7 Content2Indrani DasОценок пока нет
- Pleural EffusionДокумент72 страницыPleural Effusionmaeliszxc kimОценок пока нет
- Surgery As An Aid To More Efficient Service With Prosthetic Dentures KazanjianДокумент16 страницSurgery As An Aid To More Efficient Service With Prosthetic Dentures KazanjianJuan Sierra ZambranoОценок пока нет