Вам также может понравиться
- Prevalence of Tooth Forms and Their Gender CorrelationДокумент6 страницPrevalence of Tooth Forms and Their Gender CorrelationPablo BenitezОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Ultimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsДокумент17 страницUltimate Ceramic Veneers: A Laboratory-Guided Preparation Technique For Minimally Invasive RestorationsPablo BenitezОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Virtual Smile Design Tip: From 2D To 3D Design With Free SoftwareДокумент2 страницыVirtual Smile Design Tip: From 2D To 3D Design With Free SoftwarePablo BenitezОценок пока нет
- Dental Caries in The Second Millennium: Conference PapersДокумент7 страницDental Caries in The Second Millennium: Conference PapersPablo BenitezОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- When To Intervene in The Caries Process? An Expert Delphi Consensus StatementДокумент13 страницWhen To Intervene in The Caries Process? An Expert Delphi Consensus StatementPablo BenitezОценок пока нет
- Jopr B1Документ13 страницJopr B1Pablo BenitezОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Grupo 4 Rev1Документ4 страницыGrupo 4 Rev1Pablo BenitezОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Amalgam Vs Composite Restoration, Survival, and Secondary CariesДокумент3 страницыAmalgam Vs Composite Restoration, Survival, and Secondary CariesPablo BenitezОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- 11 - Soft Tissue Waxup and Mock-Up and Key Factors inДокумент15 страниц11 - Soft Tissue Waxup and Mock-Up and Key Factors inPablo BenitezОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Cuspal Flexure and Stress in Restored Teeth Caused by Amalgam ExpansionДокумент8 страницCuspal Flexure and Stress in Restored Teeth Caused by Amalgam ExpansionPablo BenitezОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- 10 - "Crown-then-Graft" - A Novel Approach To OptimizeДокумент14 страниц10 - "Crown-then-Graft" - A Novel Approach To OptimizePablo BenitezОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Prevalence of Cusp Fractures in Teeth Restored With Amalgam and With Resin-Based CompositeДокумент6 страницPrevalence of Cusp Fractures in Teeth Restored With Amalgam and With Resin-Based CompositePablo BenitezОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Amalgam or Composite Resin? Factors Influencing The Choice of Restorative MaterialДокумент8 страницAmalgam or Composite Resin? Factors Influencing The Choice of Restorative MaterialPablo BenitezОценок пока нет
- Periodontal Risk and Recall Interval EvaluationДокумент9 страницPeriodontal Risk and Recall Interval EvaluationPablo BenitezОценок пока нет
- CMR-MDT: Cost-Effective SolutionsДокумент3 страницыCMR-MDT: Cost-Effective Solutionshamed1725Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Case 2278Документ4 страницыCase 2278Cherie JohnsonОценок пока нет
- Utkrisht Test-6Документ5 страницUtkrisht Test-6Mayank GoelОценок пока нет
- Calculation Slab Product YardДокумент12 страницCalculation Slab Product YardNURUL IZZAHОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Fiitjee Rankers Study Material RSMДокумент3 страницыFiitjee Rankers Study Material RSMVivek Jha50% (2)
- Summative Assessment 1 2nd QuarterДокумент2 страницыSummative Assessment 1 2nd QuarterJudith DurensОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Natsha Le ChatelierДокумент5 страницNatsha Le Chatelierjefferson pabloОценок пока нет
- MeteorologyPart1 196 QДокумент193 страницыMeteorologyPart1 196 QBharat HarmilapiОценок пока нет
- Visual Examination of Welds - Welds 3-14Документ64 страницыVisual Examination of Welds - Welds 3-14carlos100% (1)
- June 2021 (v2) QP - Paper 2 CIE Physics IGCSEДокумент16 страницJune 2021 (v2) QP - Paper 2 CIE Physics IGCSEMonoОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
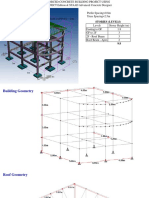
- 2 Storeys BuildingДокумент30 страниц2 Storeys BuildinglavyОценок пока нет
- Welding and Time StudyДокумент60 страницWelding and Time StudyShanky Kumar50% (2)
- O Level Notes On Mass, Weight and DensityДокумент8 страницO Level Notes On Mass, Weight and DensityRavi MothoorОценок пока нет
- DL-T 5358-2006 Technical Code For Anticorrosion of Metal Structures in Hydroelectric and Hydraulic EngineeringДокумент43 страницыDL-T 5358-2006 Technical Code For Anticorrosion of Metal Structures in Hydroelectric and Hydraulic Engineeringsaliyarumesh2292Оценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- 9 Science Experiments About Light For KidsДокумент7 страниц9 Science Experiments About Light For KidsgaylebugayongОценок пока нет
- RS6100004Документ52 страницыRS6100004e_readingОценок пока нет
- M-120 Material Data Sheets For Structural Steel Edition 5Документ47 страницM-120 Material Data Sheets For Structural Steel Edition 5vlong3003100% (3)
- Company Profile June 2022Документ26 страницCompany Profile June 2022Mark anthony GauranoОценок пока нет
- SpaceCAD Model Rocket SoftwareДокумент7 страницSpaceCAD Model Rocket Softwareheric19886445Оценок пока нет
- Is 8147Документ170 страницIs 8147Asha JatalОценок пока нет
- Mechanics Level 2Документ32 страницыMechanics Level 2greycouncil100% (1)
- Montevecchi2018heat Accumulation Prevention in Wire-Arc-Additive-Manufacturing Using Air JetДокумент9 страницMontevecchi2018heat Accumulation Prevention in Wire-Arc-Additive-Manufacturing Using Air JetGustavo de CastroОценок пока нет
- Dresser-Rand GFC Databook - Gas Field Policies-2Документ29 страницDresser-Rand GFC Databook - Gas Field Policies-2kistaiОценок пока нет
- VRMP Projects - #973 Hgu Reformer Insulation Monthly Completion Plan Project: Reformer Works - HGU-EPCC 6, HPCL, VIZAGДокумент1 страницаVRMP Projects - #973 Hgu Reformer Insulation Monthly Completion Plan Project: Reformer Works - HGU-EPCC 6, HPCL, VIZAGsusantaОценок пока нет
- Mr. Saxena - EP88Документ11 страницMr. Saxena - EP88Umar ShamshiriОценок пока нет
- 25mm de Transducer System 105826-01 Rev DДокумент74 страницы25mm de Transducer System 105826-01 Rev DHamid HannitОценок пока нет
- Nuvia Cprime Resin (Mixed-Mode Resin) Product Informatoin Bulletin - 6242Документ4 страницыNuvia Cprime Resin (Mixed-Mode Resin) Product Informatoin Bulletin - 6242Sairam EdupugantiОценок пока нет
- Bohler Welding in Tool MakingДокумент24 страницыBohler Welding in Tool MakingcfcshakerОценок пока нет
- Philippine Society of Mechanical EngineersДокумент27 страницPhilippine Society of Mechanical EngineersrollramsОценок пока нет
- Explain The Concept of Fuel Cells.: Advantages Over Conventional Energy SourcesДокумент9 страницExplain The Concept of Fuel Cells.: Advantages Over Conventional Energy SourcesAnusha AnandОценок пока нет
- The Great Bridge: The Epic Story of the Building of the Brooklyn BridgeОт EverandThe Great Bridge: The Epic Story of the Building of the Brooklyn BridgeРейтинг: 4.5 из 5 звезд4.5/5 (59)