IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 8 Ver. VIII (Aug. 2015), PP 42-51
www.iosrjournals.org
A Prospective Clinical Study of Surgical Management of Proximal
Humeral Fractures
Harish .K1, Ajith Kumar K.S2, J.K. Reddy3.
1,2,
Post graduate ( Resident) in orthopaedics, Bangalore medical college and research centre, Bangalore,
Karnataka state, India.
3
Professor and HOD in orthopaedics, Bangalore medical college and research centre, Bangalore, Karnataka
state, India.
Abstract:
Background: Treatment of proximal humerus fractures has been the subject of much controversy and
confusion. This is because of the complexity of these injuries, fracture displacements are difficult to see without
careful radiographic views and associated soft tissue injuries: Our prospective study has evaluated the
functional results of the methods of surgical management of displaced fractures of proximal end of humerus.
Materials & Methods: 20 patients with displaced fractures of proximal humerus in adults undergone surgical
management. Patients were followed from 6 weeks 15 months on OPD basis with radiological , clinical &
functional evaluation.
Results: The most common type observed in our series was three part fracture accounting for 12 of 20 patients
(60%). At the end of clinical and radiological union and full functional recovery the results were evaluated by
Neers score. Of the 20 patients 3(15%) had excellent results, 9 (45%) had satisfactory results, 6 (30%) had
unsatisfactory results and 1(5%) was a failure. 1 patient expired during follow up due to medical problems .
Conclusions: Clinical evaluation, obtaining proper radiological views, age of the patient and activity levels
holds the key for realistic approach in the management of fractures of proximal humerus. Anatomical reduction
is an essential feature in these fractures. Open reduction and internal fixation with buttress plate as well as
pinning has given good results.
Key-words: Buttress plate, Functional evaluation ,Neers score, Proximal humerus fractures ,Surgical
management.
I. Introduction
Life is Movement, Movement is life.[1] The fast pace of modern Life, acceleration of travel increases
the number of fractures. The proximal humerus fractures results from drawbacks of the fast life and violence. [2]
It consists of 2% to 3% of upper extremity fractures, incidence to be about 73 per 1,00,000 population with three
fourths occurring after the age of 60 years and women out numbering men. Fractures of proximal humerus
account for 30-40% of all humeral fractures.80% of the proximal humeral fractures are undisplaced , minimally
displaced and usually treated non-operatively generally resulting in satisfactory outcome. Remaining 20% of
fractures are significantly displaced and more difficult to manage. Fixation objectives are accompanied with a
thorough understanding of anatomical considerations, fracture personality, operative indications, surgical
exposure and fixation techniques.[3][4][5][6][7][8]
Treatment of proximal humerus fractures has been the subject of much controversy and confusion. This
is because of the complexity of these injuries, fracture displacements are difficult to see without careful
radiographic views and associated soft tissue injuries. Further, there has always been diversity of opinion about
the care of shoulder fractures, with frequent controversies and lively debate, further more even good anatomical
results achieved at operative repair may lead to poor results unless there is meticulous post operative
rehabilitation, which can be more challenging in the shoulder than operative technique. [3][4][9]
80% of proximal humerus fractures are minimally displaced and of the remainder only a few are severe
fracture-dislocations, about which much debate is centered. So with this background the title for this study was
chosen as it was essential to know the outcome and results of surgical management of proximal humeral
fractures.
II. Aims And Objectives
1.
2.
3.
To study the methods of surgical management of fractures of proximal end of humerus.
To evaluate the results of this study with respect to fracture union and restoration of shoulder function.
To evaluate fracture union and complications.
DOI: 10.9790/0853-14884251
www.iosrjournals.org
42 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
III. Materials And Methods
This prospective study was done at our institution from June 2003 to July 2005.
The protocol was
approved by the local ethics committee and written informed consent was obtained from each patient. During
this study ,20 patients with fractures of proximal humerus in adults ,that is the fractures involving surgical neck,
tuberosities greater and lesser, anatomical neck and head splitting fractures were selected. Exclusion criteria
were fractures in children, fractures in osteoporotic bones and compound fracture.
Most of the patients were brought to the casualty or admitted through out patient basis. History was
taken by verbal communication; clinical examination both local and systemic was done, careful local
examination of skeletal system and soft tissue injuries was done. Later radiological examination routine AP
view and trauma series view that is scapular AP and lateral and axillary views were done to analyze fracture
anatomy, classify and plan the mode of treatment. Arm was immobilized in U slab and arm sling.
Fractures of the proximal humerus are most commonly classified with use of system introduced by
Neer in 1970. Fractures are classified by evaluating displacement of the four principal fragments head, shaft,
greater tuberosity and lesser tuberosity. [10][11]
Indication for Surgical management was
1. Failure of closed reduction in two part fractures.
2. All displaced fractures three and four Part.
3. Fracture dislocation.
4. Fractures associated with neuro-vascular injuries
Once the general condition of the patient was stabilized pre- operative planning and baseline
investigations were done. Once patients general condition stabilized operative fixation was done, open
reduction and internal fixation was done within 8-20 days .Patients were posted for surgery under general
anaesthesia ,open reduction and internal fixation or percutaneous pinning of proximal humeral fractures or
hemi arthroplasty were done. Through delto- pectoral approach open reduction and internal fixation with
buttress plate or cloverleaf plate or cancellous screws or K-wires was done.
Post-operatively limb is immobilized in arm pouch, Mobilization was started in the second week with
pendulum exercises as per patients tolerance. Immediate post-op X-Rays were done ,routine A-P and scapular
view to assess the reduction of fracture and stability of fixation. Suture removal was done on 10th day. Patients
were discharged with arm pouch and advise to continue pendulum exercises. Patients underwent rehabilitation
as per protocol .
Patients were followed from 6 weeks -15 months on OPD basis at intervals of 6 Weeks, 12 Weeks, 6
Months ,12 months & 15 months. During this period in each visit clinical evaluation of wound healing, pain,
shoulder function and range of movements were assessed and recorded. Anatomy of the fracture was assessed
by radiographs. Fractures were assessed for clinical and radiological union. Clinically fracture was consider
united when there was no complaints from patients like residual pain, sense of insecurity, no tenderness, at the
fracture site or full function of shoulder. Radiologically fracture was regarded as united when there is no visible
fracture line. . Results were evaluated by the use of Neers shoulder score based on pain, function, range of
motion and anatomy for each case assessed and recorded.
IV. Observations And Results
In our study all cases were closed type of proximal humeral fractures.
Age group: In our series of twenty patients, four were in the age group of 21-30(20%) three in the age group of
31-40(15%), four in the age group of 41-50 (20%) seven in the age group of 51-60 (35%) and two were in the
age group of 61-70(10%).
Sex incidence :In our study, seventeen out of twenty (85%) were males and three (15%)were females.
Mode of injury :The most common observed in our series was road traffic accident. It accounted for ten of
twenty patients(50%).The next common cause was history of fall accounting for nine of twenty patients
(45%)and one patient had a history of assault(5%).
Type of fracture :The most common observed in our series was three part fracture accounting for twelve of
twenty patients (60%).The next common being two-part fracture accounting for five of twenty patients
(25%).The fracture dislocation was observed in one patient(5%). Fracture dislocation was observed in two out
of twenty patients (10%).
DOI: 10.9790/0853-14884251
www.iosrjournals.org
43 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
In our series the majority were 3 part fractures (12 patients) ,2 patients with 2 part fractures, and 1
with fracture dislocation underwent open reduction and internal fixation with buttress plate. 3 patients with 2
part fractures with failed closed reduction underwent percutaneous pinning with K-wire and cancellous screws.
1 patient with anatomical neck fracture & one with four part fracture underwent hemi arthroplasty..Most of the
cases were approached by delto pectoral approach except only in 3 cases were percutaneous pinning was done.
Fractures was anatomically reduced and fixed with T Buttress plate or Cloverleaf plate with 4.5 mm cortical
screws and 6.5mm cancellous screws for fifteen patients. Two patients underwent hemiarthroplasty with Neers
prosthesis. Three patients underwent fixation with K-wires and cancellous screws. Fixation rigidity was checked
on table. Patients were mobilized in the arm pouch.All patients were encouraged pendulum exercises in the
second week. Sutures were removed on the 10 th post operative day.
The average follow up duration has 11.6 months. Range- (10-15months). The average time taken for
clinical union was 12.8 weeks (11-16weeks) and for radiological union15.6 weeks (16 to 22 weeks).
Range Of Motion:
At the end of full functional recovery all patients assessed by Neers shoulder score had restriction of
abduction, forward flexion and external rotation. The average loss of abduction was 67, forward flexion 60,
external rotation was 17, internal rotation 15, extension 12. The average range of movements observed was
abduction 113 , forward flexion 120, extension 33, external rotation 28, internal rotation 54.5.
Evaluation Of Results By Neers Shoulder Score:
At the end of clinical and radiological union and full functional recovery the results were evaluated by
Neers score. Of the twenty patients three (15%) had excellent results, nine (45%) had satisfactory results, six
(30%) had unsatisfactory results and one (5%) was a failure. One patient expired during follow up due to
medical problems.
Complications:
During the follow up period four patients had post-operative infection(20%) , six patients had shoulder
stiffness(30%) and one patient had implant loosening(5%) and had to undergo revision in which case cementing
was done.. There were no incidences of non-union, malunion & osteonecrosis of the proximal humerus.
V. Discussion
Proximal humeral fractures constitute 4-5% of all fractures of long bones. It constitutes for 2-3% of the
fractures of upper limb. 75% of these fractures are seen in elderly. 80-85% of these fractures are amenable to
conservative treatment remaining 15-20% are significantly displaced and require some type of internal fixation
.[4][9][12]
In this study at our institution, 20 patients with fractures of proximal humerus were managed by open
reduction and internal fixation through the delto pectoral approach .Out of the 20 patients, 15 were treated with
buttress plate, 3 with K.wires and cancellous screw and 2 underwent hemiarthroplasty.
Indications for surgery in our series were
1. Failure of closed reduction in two part fractures.
2. All displaced fractures three and four part (>1 cm displacement and > 45 angulation ).
3. Fracture dislocations.
Age Incidence
The average age incidence in our series was 46.4 years, which was consistent with the age incidence in
studies done by Neer was 55.3 years.[9][10] In other studies the average age was 52 year.[13] In our series 11 out
of 20 patients were below the age of 50 years and hence the average age incidence was 46.4 years in our series.
Sex Incidence
Regarding sex incidence study of literature reveals predominance of proximal humeral fractures in
females in an elderly age group.[3] Studies also reveal that male to female ratio being 1:0.8 [13]and 1:1.3 [6] .In
our series the male to female ratio is 1:0.2, 17 among 20 patients were males. The reason for high incidence of
males in our series being that the majority of the cases, 11 out 20 were within the age of 50years and 8 among
them were less than 40 years of age. These fractures of proximal humerus have bimodal presentation with
adolescents and younger middle age who are more prone for high velocity injuries most common among males
forming one group and later these fractures are seen in elderly patients(>50 years) in which cases they are
osteoporosis related most often seen in females.[2]
DOI: 10.9790/0853-14884251
www.iosrjournals.org
44 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
Mode Of Injury
The mode of injury commonly observed in our series was road traffic accidents accounting for 10
(50%),9 (45%) patients had an history of fall and 01(5%) had an history of assault. These observations was
found to be consistent with the studies in literature which revealed 19(45%) road traffic accidents,20(50%)
history of fall and 01(5%) history of assault out of the forty cases studied ... [6][13] In another study 12(75%) had
road traffic accident and 04(25%) had history of fall in a series of 16 cases studied. [6]
Type Of Fracture
The study of type of fracture in our series revealed 7(35%) were 2 part fractures, 12(60% were 3 part
fractures and 01 (5%) was a 4 part fracture. In studies done by Neer 9,10 in a series of 117 patients studied
31(26.5%) were 2 part fractures, 43(36.8%) were 3 part fractures and 43(36.8%) were 4part fractures. In another
study of 40 cases 20(50%) were 2 part fractures, 16(40%) were 3 part fractures and 4(10%) were 4 part fractures
indicating that the incidence of type of fracture is nearly consistent with the studies in literature. [13]
Modes Of Internal Fixation
Different modes of internal fixation was employed in our series of 20 patients 15(75%) underwent open
reduction and internal fixation with buttress plate, 03(15%) underwent fixation with K-wires and cancellous
screws and 02(10%) underwent prosthetic replacement. In study of literature 117 cases studied by Neer
43(36.8%) underwent open reduction and internal fixation with buttress plate and tension band
wiring,43(36.8%) of 4 part fractures and selected 3 part fractures underwent prosthetic replacement. 9,10. In
another series of 15 patients 14(93.3%) underwent internal fixation with K-wires/cancellous screws and only
one underwent fixation with AO buttress plate..[6]
Follow Up
All fractures united with in one year the mean follow up period was 11.6 months during which clinical
evaluation was done for clinical union, radiological union and functional assessment was done. All fractures
revealed clinical union at 12.8 weeks (11-16weeks). Like wise radiological union was assessed which was
noticed 15.6weeks (16-22 weeks). Literature reveals the average clinical union time for minimally invasive
procedure being 8 -10 weeks and for OR & IF with plates 12-14 weeks.[6][7][13]
Range Of Motion
Range of motion at the end of full follow up period was assessed regarding the movements of
abduction, forward flexion, internal rotation, external rotation and extension. In our series the average values for
the above shoulder movements were abduction 113 , forward flexion 120, Internal rotation 54.5, external
rotation 29 and extension 33. These results compared with the studies on percutaneous fixation are
satisfactory.[6][7] The reasons for difference in observed values are probably due to poor surgical technique,
increased soft tissue handling in open reduction and internal fixation and lack of awareness or understanding the
importance of rehabilitation programme in our patients.
Results
The results in our series of patients were evaluated with the use of Neers criteria for different types of
fixation and analyzed with other studies. In our series 15 cases of three part fractures treated with OR & IF had
01 (5%) excellent results, 08 (40%) had satisfactory results, 05 (25%) had unsatisfactory results and 01(5%) was
a failure. When compared with other studies in case of Neers 30 cases, 19 cases (63.3%) had excellent and
satisfactory results .[9][10]
In other study of 15 cases of 3 part fracture 14 (93.3%) had excellent and
satisfactory results, all of them had underwent OR & IF with K wires/cancellous screws and one failure in this
series was fixation with AO buttress plate. In Neers series 11 cases (36.7%) was a failure compared with our
series in which case we had 30% of unsatisfactory and failure results. This implies that our results with OR & IF
are almost correlated with the studies in literature but improved results are seen in minimal fixation techniques.
Studies reveal that results of percutaneous pinning are more superior to OR & IF regarding functional
outcome. In 48 cases studied 91.6% of the cases had excellent (70.8%) and satisfactory (20.8%) results with 04
(8.3%) failures.[14] In our series two patients underwent percutaneous pinning both had excellent results.
Results pertaining to prosthetic replacement , studies reveal that prosthetic replacement is of chores in 4
part fracture and selected 3 part fracture in elderly. Neer studied 43 cases of which 5 (11.6%) had excellent ,34
(79%) had satisfactory results only 4 had unsatisfactory and failure. 10In another study of 70 patients 31(44.3%)
had excellent results, 22(31.4%) had satisfactory results and 17 (24.3%) had unsatisfactory results. In our series
of 20 patients 02 underwent prosthetic replacement one with anatomical neck fracture and other patient with
four part fracture. We had one satisfactory result and one unsatisfactory result. The unsatisfactory results was
due to implant loosening, she had to undergo revision surgery with bone cementing.
DOI: 10.9790/0853-14884251
www.iosrjournals.org
45 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
In the overall results analyzed in our series 60% of the patients had excellent and satisfactory results
and 35% had unsatisfactory and failure outcome. This was observed to be on par with the studies in literatures
.[6][7][13][14]
The unsatisfactory results in our series was seen mostly in elderly patients who had metaphyseal defect
and in which cases bone grafting was not done thus delaying the union time. These patients were reluctant or not
compatible for rigorous rehabilitation programme. Decreased immunity status lead to infection in few of these
patients resulting in unsatisfactory and failure outcome.
Complications
Complications following surgeries on proximal humerus is seen most of the time due to poor surgical
technique, decreased patient compliance and lack of good rehabilitation programme. In our series 06(30%) had
shoulder stiffness,04(20%) had post operative infection and 01(5%) had implant loosening. Compared to other
series [7][9][10] we had stiffness in 30 % of the patients, most of these patients were elderly who were unwilling
to undergo rigorous rehabilitation programme. 20% of our patients had post operative infection ,3 of them had
superficial infection which subsided with systemic antibiotics but one patient had deep seated infection after
discharge from hospital but reported late to hospital after 3 weeks, for whom aspiration was done and later
subsided by systemic antibiotics who later developed arthritis of shoulder and accounted for failure outcome,
other three patients had unsatisfactory results. One patient who underwent hemiarthroplasty had recurrent
subluxation of the implant due to implant loosening, after 3 months she underwent revision surgery in which
case the implant was reinforced with bone cement and S.S wire fixation for the tuberosity. The complications in
other series seen were in a series of 117 patient studied by Neer
03 had post operative infection , 04 had
malunion ,07 had non union and 08 had avascular necrosis of the humeral head .[9][10 ]
In another series of
15 patients 2 had implant loosening and 2 had avascular necrosis of the humeral head . [7]
VI. Conclusion
In conclusion, fracture of the proximal humerus is still a debatable and controversial subject in
orthopaedics.Clinical evaluation, obtaining proper radiological views, age of the patient and activity levels holds
the key for realistic approach and proper surgical management of these complex fractures .
Anatomical reduction is an essential feature in these fractures. Open reduction and internal fixation with
buttress plate as well as percutaneous pinning has given good results. Rehabilitation to achieve good functional
recovery of the shoulder is very essential especially in middle aged and elderly individuals following any mode
of fixation. With results assessed with standard shoulder scoring system of Neers, we have achieved 60% of
excellent and satisfactory results,30% unsatisfactory and 10% failure outcome.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
[14].
M.E.Muller, M.Allgover, R.Schneider, H .Willenegger et al . Manual of internal fixation: Techniques recommended by AO/ASIF
Group .3rd Ed 2002 Springer-VerlagBerlin Heidelberg Newyork Tokyo pg 438-441.
Steven .H.Rose Joseph Melton Bernard.F.Morrey et al. Epidemiological features of
humeral fractures. Clin. Orthop1982:168:24-30.
Terry Canales Campbells Operative Orthopaedics. Vol-3: 9th edition , 1998 Mosby Publishers, USA Pg 2286-2296
Bucholz and Heckmans Rockwood &Greens Fractures in Adults. Vol-1: 5th Ed 2001, Lippincott Williams and Wilkins Company,
USA Pg 1055-1107.
Hawkins RJ, Kiefer Gin et al. Internal fixation for proximal humeral Fractures .Clin. Orthop-1987:223:77-85.
6. Kojy, Yamamoto R et al. Surgical Treatment of complex fractures of the proximal humerus. Clin.Orthop-1996:327:225-237
7. Richard .J Hawkins , Robert.H.Bell, Kevin Gurr et al.The three part fractures of proximal part of humerus .JBJS (am) 1986: 68A:1410-14.
Robert.H.Cofield.Comminuted fractures of proximal humerus.Clin.Orthop1988:230:49-57.
Neer C.S . Displaced proximal humeral fractures Part-I Classification and Evaluation.
JBJS (am) 1970:52:1077-1089.
Neer C.S. Displaced proximal humeral fractures Part-II Treatment of three and four part displacement .JBJS (am) 1970:52:10901101.
P.Hoffmeyer. The operative management of displaced fractures of the proximal humerus . JBJS (Br) 2002 May Vol 84-B No 4 Pg
469-80.
Terry Canales Campbells Operative Orthopaedics. Vol-3: 9th edition , 1998 Mosby Publishers, USA Pg 2286-2296.
Dolfi Herscovici Jr,Darrick.T, Saunders,Marie.P.Johnson,et al . Per-cutaneous fixation of proximal humeral fractures
.Clin.Orthop2000:375:97-104.
Hans Jaberg, Jon JPWarner, Roland.P.Jacob . Percutaneous stabilization of unstable fractures of humerus .JBJS (br)1992April:Vol
74A No4:508-515.
DOI: 10.9790/0853-14884251
www.iosrjournals.org
46 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
Evaluation Of Results By Neers Shoulder Score ( Table -1)
Sl no.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
PAIN
35
35
35
35
30
35
30
35
35
expired
35
35
35
35
35
35
35
35
35
35
FUNCTION
24
22
28
30
20
30
13
20
26
RANGE OF MOTION
17
17
19
17
14
19
12
14
15
ANATOMY
8
8
8
10
8
10
4
8
8
TOTAL
84
82
90
92
72
94
59
77
84
26
24
18
26
18
22
20
20
22
22
17
17
13
18
11
15
13
13
15
15
8
8
4
8
8
8
8
8
8
8
86
84
70
87
72
80
76
76
80
80
PAIN
40
30
20
10
19
17
15
13
11
RANGE OF MOTION
20
15
10
5
15
17
19
15
17
19
13
11
FUNCTION
40
30
20
10
DOI: 10.9790/0853-14884251
13
11
www.iosrjournals.org
47 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
Type Of Fracture (Table -2)
TWO PART FRACTURE
THREE PART FRACTURE
FOUR PART FRACTURE
FRACTURE DISLOCATION
05
12
01
02
14
12
10
8
Series1
6
4
2
0
TWO PART
FRACTURE
THREE PART
FRACTURE
FOUR PART
FRACTURE
FRACTURE
DISLOCATION
Mode Of Internal Fixation (Table -3)
BUTRESS PLATE
PERCUTANEOUS PINNING
HEMIARTHROPLASTY
HEMIARTHROPLAS
TY
PERCUTANEOUS
PINNING
Series1
BUTRESS PLATE
16
14
12
10
8
6
4
2
0
15
03
02
Complications (Table 4)
Stiffness
Post op infection
Implant loosening
Malunion
Nonunion
Osteonecrosis
DOI: 10.9790/0853-14884251
06
04
01
00
00
00
www.iosrjournals.org
48 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
7
6
5
4
3
Series1
2
1
ro
sis
ne
c
os
teo
no
nu
ni
on
alu
ni
M
oo
se
ni
nt
l
on
ng
n
tio
Im
pl
a
in
fe
c
Po
st
op
St
iff
ne
ss
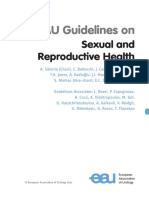
Case 1
FIG 1: pre op x-ray: three part fracture
FIG 2:Post op x-ray at 6 weeks
DOI: 10.9790/0853-14884251
www.iosrjournals.org
49 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
FIG 3:Follow up at 6 months
Case 2
Fig 3 :PRE-OP X-Ray: anatomical neck fracture
FIG 4:post op x-ray revealing prosthesis insertion
DOI: 10.9790/0853-14884251
www.iosrjournals.org
50 | Page
A Prospective Clinical Study Of Surgical Management Of Proximal Humeral Fractures
Case 3
FIG:5-Pre-op x-ray:three part fracture
FIG 6: post op x ray -Fixation with K-wires and cancellous screws
DOI: 10.9790/0853-14884251
www.iosrjournals.org
51 | Page
Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationДокумент6 страницKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Surgical Informed Consent FormДокумент2 страницыSurgical Informed Consent FormMenGuitar100% (1)
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Документ15 страницA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Оценок пока нет
- Assessment of The Implementation of Federal Character in Nigeria.Документ5 страницAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Оценок пока нет
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityДокумент5 страницAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanДокумент7 страницSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Оценок пока нет
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweДокумент5 страниц"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Оценок пока нет
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionДокумент6 страницThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Оценок пока нет
- The Impact of Technologies On Society: A ReviewДокумент5 страницThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehДокумент4 страницыInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesДокумент7 страницComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Оценок пока нет
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeДокумент7 страницA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsДокумент5 страницRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Classical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahДокумент9 страницClassical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Importance of Mass Media in Communicating Health Messages: An AnalysisДокумент6 страницImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshДокумент7 страницTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Human Rights and Dalits: Different Strands in The DiscourseДокумент5 страницHuman Rights and Dalits: Different Strands in The DiscourseInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysДокумент5 страницEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Оценок пока нет
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyДокумент14 страницAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Beowulf: A Folktale and History of Anglo-Saxon Life and CivilizationДокумент3 страницыBeowulf: A Folktale and History of Anglo-Saxon Life and CivilizationInternational Organization of Scientific Research (IOSR)Оценок пока нет
- The Lute Against Doping in SportДокумент5 страницThe Lute Against Doping in SportInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Women Empowerment Through Open and Distance Learning in ZimbabweДокумент8 страницWomen Empowerment Through Open and Distance Learning in ZimbabweInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Transforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweДокумент9 страницTransforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Role of Madarsa Education in Empowerment of Muslims in IndiaДокумент6 страницRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- An Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsДокумент6 страницAn Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Substance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaДокумент11 страницSubstance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesДокумент5 страницDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalОценок пока нет
- Motivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweДокумент8 страницMotivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Design Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextДокумент6 страницDesign Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Micro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaДокумент3 страницыMicro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- A Study On The Television Programmes Popularity Among Chennai Urban WomenДокумент7 страницA Study On The Television Programmes Popularity Among Chennai Urban WomenInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Maxillomandibular Advancement and Tracheostomy For Morbidly Obese Obstructive Sleep Apnea: A Systematic Review and Meta-AnalysisДокумент12 страницMaxillomandibular Advancement and Tracheostomy For Morbidly Obese Obstructive Sleep Apnea: A Systematic Review and Meta-AnalysisNaye Gmen DezОценок пока нет
- Abdomen 2Документ22 страницыAbdomen 2carlosОценок пока нет
- Fellowships For OphthalmologistsДокумент1 страницаFellowships For OphthalmologistsfatmaОценок пока нет
- Sample Student Results & Verification LettersДокумент3 страницыSample Student Results & Verification LettersJennybabe PetaОценок пока нет
- Nervio FacialДокумент3 страницыNervio FacialAngélica Valenzuela AndrighiОценок пока нет
- Clínica SAFДокумент29 страницClínica SAFTra21798siempreОценок пока нет
- Basic Life Support (BLS)Документ67 страницBasic Life Support (BLS)Mohamad El SharОценок пока нет
- Dapus PlastikДокумент3 страницыDapus PlastikDAN_tijalikeuhОценок пока нет
- Abstractbook2020 2Документ50 страницAbstractbook2020 2alpaslan alkanОценок пока нет
- 4.special Methods and Clinical Identification in Digestive SystemДокумент37 страниц4.special Methods and Clinical Identification in Digestive SystemToafan MegaОценок пока нет
- Resume - Viroja Sweta For PortfolioДокумент1 страницаResume - Viroja Sweta For Portfolioapi-608195339Оценок пока нет
- Contemporary Implant Dentistry: Chapter 14 of Contemporary Oral and Maxillofacial Surgery By: DrarashkhojastehДокумент65 страницContemporary Implant Dentistry: Chapter 14 of Contemporary Oral and Maxillofacial Surgery By: DrarashkhojastehRawa Omar100% (1)
- Case Study Amar LatestДокумент131 страницаCase Study Amar LatestAmar Nur Arif ZazuliОценок пока нет
- The Korean 4 Point SystemДокумент1 страницаThe Korean 4 Point SystemHuib SalomonsОценок пока нет
- 2nd Preparatory Course OMFSДокумент2 страницы2nd Preparatory Course OMFSkhurramnadeemОценок пока нет
- Stellaris Posterior OPДокумент219 страницStellaris Posterior OPMohamed AbdulaalОценок пока нет
- Iatrogenic Injury To The Internal Iliac Vein 2008Документ4 страницыIatrogenic Injury To The Internal Iliac Vein 2008waldemar russellОценок пока нет
- B Lynch SuturingДокумент32 страницыB Lynch SuturingDoru Draghici67% (3)
- Bioinstrument 5 (BP-Sound)Документ94 страницыBioinstrument 5 (BP-Sound)vividmeОценок пока нет
- Periodontal Surgery: Treatment of Multi-Rooted TeethДокумент6 страницPeriodontal Surgery: Treatment of Multi-Rooted TeethYuttapol PimpisonОценок пока нет
- Madelung's Deformity of The Wrist-CurrentДокумент4 страницыMadelung's Deformity of The Wrist-CurrentAnonymous bUBXIFfОценок пока нет
- Osteotomy at Low-Speed Drilling Without Irrigation Versus High-Speed Drilling With Irrigation: An Experimental StudyДокумент6 страницOsteotomy at Low-Speed Drilling Without Irrigation Versus High-Speed Drilling With Irrigation: An Experimental Studyanilsamuel0077418Оценок пока нет
- Cmaxs Cmaxt UkДокумент33 страницыCmaxs Cmaxt UkViniciusОценок пока нет
- EAU Guidelines On Sexual and Reproductive Health 2021Документ282 страницыEAU Guidelines On Sexual and Reproductive Health 2021Natacha CabeteОценок пока нет
- Management of Obstructive Sleep Apnea: A Dental Perspective: Eview RticleДокумент9 страницManagement of Obstructive Sleep Apnea: A Dental Perspective: Eview RticleFourthMolar.comОценок пока нет
- DiabeticRetPPP2014 SummaryBenchmarkPagesДокумент2 страницыDiabeticRetPPP2014 SummaryBenchmarkPageskomite medikОценок пока нет
- Benefit Schedule HygeiaДокумент3 страницыBenefit Schedule HygeiaAdekanbi oluwaseunОценок пока нет
- Daftar PustakaДокумент2 страницыDaftar PustakaSherly WahyuniОценок пока нет
- First Middle East Experience WДокумент8 страницFirst Middle East Experience WAsmat BurhanОценок пока нет