IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 9 Ver. III (Sep. 2015), PP 12-20
www.iosrjournals.org
Anorectal Melanoma: Radiologic-Pathologic Correlation
Amrendra Kumar Deo, Xiu-Hong Shan, Jian-Hua Chen1,
Departments of Radiology and 1Pathology, The Affiliated RenminHospital of Jiangsu University, Zhenjiang,
Jiangsu Province, P. R. China
Abstract: Anorectal melanoma is a rare but aggressive disease. Because the patients often present with nonspecific complaints, a high clinical suspicion is important to avoid a delayed diagnosis. It typically presents in
the seventh or eighth decade of life with non-specific complaints such as rectal bleeding or anal pain. A timely
diagnosis of anal melanoma is made even more difficult by the fact that most of the lesions lack obvious
pigmentation and are even histologically amelanotic. Prognosis is very poor. Anorectal malignant melanomas
spread along submucosal planes and are often beyond complete resection at the time of diagnosis. We present
the radiological and pathological features seen in the three cases diagnosed with melanoma of rectum.
Key words: Anorectal melanoma, Imaging, Wide local excision, Abdominoperineal resection, Chemotherapy.
I.
Introduction
Anorectal melanoma is a rare but aggressive disease.[1] It is difficult to diagnose clinically, due to the
non-specific symptoms and because it shows as a non-pigmented lesion in one third of cases.[1] Prognosis is
very poor with a median survival of 24months and a 5-year survival of 10-15%.[9,12] Presently, there is no
consensus on which surgical approach is favorable.[6] Anorectal malignant melanomas spread along submucosal
planes, therefore, they are often beyond complete resection at the time of diagnosis. [13]
II.
Epidemiology
The incidence of Anorectal melanoma has been doubled in the last 20 years with 1-2 cases per 1000000
populations in western countries.[1,2] Anorectal melanoma constitutes less than 1% (0.1%-4.6%) of all anorectal
malignancies and less than 1%-2% of entire melanomas.[1,4-6]90% of melanomas reside in the skin; the
remaining 10% is split between ocular melanoma (5%), melanoma of unknown origin (2%), and mucosal
melanoma (3%). Among these, Anorectal melanoma is the third most common site, after the head/neck and the
female genital system[2]. However, among primary melanomas residing in the gastrointestinal tract, the anorectal
location is the most common.[7]
Anorectal melanoma has female predominance, with 1.5:1 female to male
ratio[1,4,6], although some authors claim that this small increase results from perineal scans being more common
among females[6]. This disease usually affects elderly patients.
III.
Clinical Symptoms
Anorectal melanoma presents with symptoms perfectly attributable to benign and much more common
anorectal entities: rectal bleeding is the most common symptom, present in 53%-96% of patients, followed by
the presence of a lump or mass, tenesmus, and more sporadically, itching, change in bowel habits or
proctalgia.[1,4,5,7] Associated symptoms, of banal appearance, will continue for an average of 3-8 months until
the final diagnosis, and entails a misdiagnosis rate close to 55%. [4] Anatomically, the majority of anorectal
melanomas are located in the anal canal or in the dentate line. Only 2%-5% reside exclusively in the rectal
mucosa.[4] Usually, they are tumors (pigmented or otherwise) of 2.9-3.8 cm in diameter[3] with an ulcerated, flat
or polypoid appearance. A pigmented and polypoid lesion can be easily mistaken for a thrombosed hemorrhoid.
Indeed, in an extensive review of the Memorial Sloan-Kettering Cancer Center (MSKCC), 8% of Anorectal
melanoma diagnoses were performed after pathologic examination of hemorrhoidectomy parts; therefore, it is
recommended to systematically analyze all resected specimens and send them, identified topographically, to the
pathologist.[7,8]
Case histories
Case 1
A 79-year-old male presented with a 5-month history of a painful mass protruding from the anus with
bleeding from the rectum and alteration of bowel habit. His medical history was unremarkable. A digital rectal
examination revealed a hemorrhagic, soft mass of rectum.
DOI: 10.9790/0853-14931220
www.iosrjournals.org
12 | Page
Anorectal Melanoma: Radiologic-Pathologic Correlation
Radiological Features
A computed tomographic scan of the pelvis revealed irregular thickening of the rectal wall, soft tissue
mass arising from the rectal mucosa in the lumen. The mass showed moderate enhancement and homogeneity
on contrast-enhanced CT scan image (Fig.1A, Fig.1B, Fig.1C).
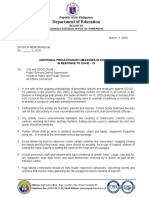
Fig.1A.Case1: Plain CT scan imageof the pelvis showing a soft tissue mass arising from the rectal mucosa in the
lumen (white solid arrow).
Fig.1B.Case1: Contrast-enhanced CT scan image of pelvis showing the soft tissue mass moderate enhancement
and homogeneity (white solid arrow).
DOI: 10.9790/0853-14931220
www.iosrjournals.org
13 | Page
Anorectal Melanoma: Radiologic-Pathologic Correlation
Fig.1C.Case1:Contrast-enhanced coronal CT scan image of pelvis showing the soft tissue mass connecting with
rectal mucosa (white solid arrow).
Pathological Features
Microscopic evaluation of the tumoral biopsy fragments showed a high-grade, necrotic malignant
tumor with scant vital tissue (Fig.1D). Areas with preserved architectural and cytologic details featured
malignant epithelioid tumors growing in solid sheaths, with irregular polygonal nuclei and glassy cytoplasm.
Immuno-histochemical examination showed tumor cells positive for S100, HMB45 and Melan-A.
Fig.1D.Case1: Fragments of rectal mass showing coagulative necrosis and scant fragments of viable tissue,
including shreds of tumor cells and a few mucous glands.
Case 2
A 61-year-old female presented with a 2-month history of bleeding from the rectum and alteration of
bowel habit. She was a hypertensive patient under medication. A digital rectal examination revealed a
hemorrhagic, soft mass of rectum.
Radiological Features
A computed tomographic scan of the pelvis revealed local irregular thickening of the rectal wall,
findings consistent with colorectal cancer and a small node arising from rectal mucosa. The node showed
moderate enhancement on contrast-enhanced CT scan image (Fig.2A, Fig.2B, Fig.2C).
DOI: 10.9790/0853-14931220
www.iosrjournals.org
14 | Page
Anorectal Melanoma: Radiologic-Pathologic Correlation
Fig.2A.Case2: Plain CT scan image of the pelvis showing a small node arising from the rectal mucosa (white
solid arrow).
Fig.2B.Case2: Contrast-enhanced CT scan image of the pelvis showing the node moderate enhancement (white
solid arrow).
Fig.2C.Case2: Contrast-enhanced coronal CT scan image of the pelvis showing the node connecting with rectal
mucosa (white solid arrows).
DOI: 10.9790/0853-14931220
www.iosrjournals.org
15 | Page
Anorectal Melanoma: Radiologic-Pathologic Correlation
Pathological Features
Microscopic evaluation of thetumoral biopsy fragments revealed pleomorphic lesions displaying high
mitotic rate and prominent nucleoli. It showed intra- and extra-cellular melanin pigment on microscopic
examination (Fig.2D).
Immuno-histochemical examination showed tumor cells positive for S100, HMB45 and Melan-A.
Fig.2D.Case2: Histopathological biopsy sample shows pleomorphic lesions with melanin pigment.
Case 3
A 74-year-old female presented with a 4-month history of bleeding from the rectum and alteration of
bowel habit. She was non-smoker with unremarkable medical history. A digital rectal examination revealed a
hemorrhagic soft mass of rectum.
Radiological Features
A computed tomographic scan of the pelvis revealed partial bowel wall thickening and dilatation of
intestine at the sigmoid colon with small lymph nodes around and abdominal aortic wall calcification (Fig.3A,
Fig.3B, Fig.3C).
Fig.3A.case3: Plain CT scan image of the pelvis showing partial bowel wall thickening and dilatation of
intestine at the sigmoid colon (white solid arrow) with small lymph nodes around.
DOI: 10.9790/0853-14931220
www.iosrjournals.org
16 | Page
Anorectal Melanoma: Radiologic-Pathologic Correlation
Fig.3B.case3: Contrast-enhanced CT scan image of the pelvis showing the tumor slightly enhanced
homogenously (white solid arrow).
Fig.3C.case3: Contrast-enhanced coronal CT scan image of the pelvis showing partial bowel wall thickening
and dilatation of intestine at the sigmoid colon (white solid arrow).
Pathological Features
Histopathological biopsy sample of the rectal mass showed atypical polygonal cells with frequent
mitotic figures (Fig.3D). Areas of coagulative necrosis were common.
Immuno-histochemical examination showed tumor cells positive for S100, HMB45 and Melan-A.
DOI: 10.9790/0853-14931220
www.iosrjournals.org
17 | Page
Anorectal Melanoma: Radiologic-Pathologic Correlation
Fig.3D.case3: Biopsy sample of the rectal mass showing atypical polygonal cells with stainable cytoplasm,
hyperchromatic nuclei and smudged chromatin.
IV.
Discussion
All melanomas, whether cutaneous or mucosal in origin, originate from melanocytes, which are cells
derived from the embryological neural crest. During fetal development, these cells migrate to many sites
throughout the body, primarily to the skin. However, melanocytes also reside in the eyes (retina and uveal tract)
and mucosal surfaces.[6,10] Therefore, cutaneous melanomas are by far the most common form of the disease,
comprising more than 90% of all melanomas. Of the remaining 10% forms of melanoma, ocular melanoma
accounts for 5%, melanoma of unknown origin for 2%, and mucosal melanoma for 3%. Melanocytes may
undergo malignant transformation when exposed to ultraviolet UVB light, which is a carcinogenic stimulus.
However, this relationship is not apparent in anorectal melanoma. [13] There is a likely role of
immunology in the development of anorectal melanoma as the incidence is higher in patients with Human
Papilloma virus (HPV) and Human Immunodeficiency virus (HIV) infections.[13,14] In the rectum, melanocytes
are located at the anal transition zone and squamous zone. Most anorectal melanomas arise from the dentate line
and 65% are located within the anal canal or at the anal verge. [6,13] The most common presenting complaints are
bleeding, anorectal discomfort or pain, an appreciable anorectal mass, or change in bowel habits. Other
symptoms include pruritis, tenesmus, prolapsed hemorrhoid, change in stool habits, and diarrhea. Patients who
have metastasis at the time of presentation may additionally have fatique, weight loss, and anemia. [6,13] Lesions
are most commonly found at the anorectum, followed by the anal canal and anal verge. [11] These lesions are
often discounted as being benign hemorrhoids or polyps.[12,13]
A sigmoido-colonoscopy is essential both for evaluation of the cause of symptoms and obtaining a tissue biopsy
from a suspicious lesion. Endoscopic endorectal ultrasound may be considered to evaluate tumor thickness and
surrounding nodal status.[13]
Computed tomography (CT) scan of the abdomen and pelvis is not the preferred diagnostic modality to
evaluate hematochezia or alteration in bowel habit, but is a valuable tool to assess regional disease, and is
frequently utilized to determine if there is lymphadenopathy or metastasis once neoplasia is suspected.[10,12,13]
Contrast-enhanced CT scan and MRI allow characterization and assessment of the extent of the tumor. On CT
scans, primary rectal malignant melanomas appear as bulky intraluminal fungating masses in the distal rectum,
focally expanding and obscuring the lumen without causing obstruction, with perirectal infiltration and
frequently enlarged lymph nodes.[15] Rectal carcinoma or other rectal masses present as significant obstruction.
In our cases, irregular thickening of the rectal wall was the common CT finding.
MRI shows the melanotic component as high signal intensity on T1-weighted imaging and mixed
signal intensity on T2-weighted imaging.[16]Extraluminal extent of the lesion is better demonstrated by MRI
imaging. Other rectal mass lesions show hypointense signal on T1-weighted imaging.
In cases of diagnostic difficulty, which is frequent even on histopathology, the presence of melanin can
be helpful, but it is not easily detected in anorectal disease. [13]In our cases, presence of melanin was a diagnostic
marker. Melanoma antigens S-100, HMB-45, and vimentin are important immuno-histochemical markers. In
our cases, immuno-histochemical examination showed tumor cells positive for S100, HMB45 and Melan-A.
Polyclonal antiserum and monoclonal antibodies to carcinoembryonic antigen can help to distinguish it from a
poorly differentiated epidermoid carcinoma.[10,13] Activating KIT-gene mutations, which are implicated in
leukemia and gastrointestinal stromal tumors have been associated with the pathogenesis of malignant
melanoma.[6]
Malignant melanoma of the rectum is a rare and very aggressive rectal tumor. [9] Lymphatic spread to
the inguinal or inferior mesenteric node is common. The most common sites for metastases are inguinal lymph
DOI: 10.9790/0853-14931220
www.iosrjournals.org
18 | Page
Anorectal Melanoma: Radiologic-Pathologic Correlation
nodes, mesenteric lymph nodes, hypogastric lymph nodes, para-aortic lymph nodes, liver, lung, skin and
brain.[10] The incidence rates for locoregional lymph node metastases on initial presentation are almost 60%. [9,10]
At the time of diagnosis, distant metastases are identified in 26-38% of patients.[6,10]
Anal melanoma is staged on a clinical basis, focusing on loco-regional and distant spread. Stage I is
local disease only, Stage II is a local disease with increased thickness and ulcerations, Stage III is local disease
with involvement of regional lymph nodes, and Stage IV shows distant metastatic disease.[10,13]
The treatment of anal melanoma, unfortunately, is only moderately successful. Surgery remains the
cornerstone of treatment.[9,10] Of all patients diagnosed with anorectal melanoma the 5-year survival rate can
range from 16 to 34%. In patients who have metastasis at the time of diagnosis, the disease-free survival rate
may drop to 16% from 22%.[6,13] The controversy has been whether abdominoperineal resection (APR) is
needed or wide local excision (WLE) is adequate for complete treatment. APR, although a highly morbid
operation, has long been thought to be the best means of control of anorectal melanoma. Lately, there has been a
paradigm shift after several studies indicated that WLE may be adequate to control disease, while minimizing
the morbidity of surgery because anorectal melanoma is a systemic disease at the time of diagnosis and no
surgical treatment, regardless of how aggressive, will truly change the outcome.[6,9,10,13] The benefits of a WLE
are quicker recovery, no need for a stoma, and minimal impact on bowel function.[13] Lymph node dissection
may be indicated in clinically apparent disease or for occult disease identified with sentinel lymph node (SLN)
techniques.[6,10]
There are no standards regarding systemic therapy for disseminated disease. Chemotherapy, radiation
therapy, and immune therapy have a limited role. The medications used in adjuvant therapy are cisplatin,
vinblastine, dacarbazine, interferon B, and Interleukins IL-2-8. Dacarbazine is the most commonly used single
agent and usually initiates a partial response in 20% of patients in 4-6 months after treatment.[10,13] Recent
studies show that wide local excision (WLE) combined with adjuvant loco-regional radiotherapy result in
comparable loco-regional control with less loss of function compared to APR.[9]
The rarity of this disease and the limited number of patients who present with early disease, have
prevented definitive trials examining the optimal treatment of curable anal melanoma. [6,10,12,13]
V.
Conclusion
Anorectal melanoma is extremely rare, highly aggressive, and difficult to diagnose. Bulky fungating
masses in the distal rectum obscuring the lumen without causing significant obstruction seen on CT and MRI
scans raise the possibility of anorectal malignant melanoma. On MRI, the melanotic component of rectal mass
can be seen as high-signal intensity on T1-weighted imaging further strengthening the diagnosis. Although
biopsy and histopathological examination are essential for diagnosis, distinct radiological features on CT, and
MRI may suggest the possibility of malignant melanoma. Major role of CT and MRI is in preoperative staging
of the tumor.
Although surgery remains the cornerstone of treatment, the exact procedure remains controversial. Role of
adjuvant therapies is minimal. The delayed diagnosis of anorectal mucosal melanoma (ARMM) leaves a poor
prognosis and a standardized evidence-based treatment approach is not well-defined due to the rarity of this
disease.[17]
The only hope of improved survival lies in early diagnosis and treatment. Since, the complaints are
usually non-specific; this is only possible with a high index of suspicion followed by early sigmoidoscopy and
biopsy.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
Merguerditchian A, Meterissian SH, Bullard Dunn K. Anorectal melanoma: diagnosis and treatment. Dis Colon Rectum.
2011;54:638-44.
Nilsson PJ, Regnarsson-Olding BK. Importance of clear resection margins in anorectal malignant melanoma. Br J Surg.
2010;97:98-103.
Pessaux P, Pocard M, Elias D, Duvillard P, Avril MF, Zimmerman P, et al. Surgical management of primary anorectal melanoma.
Br J Surg. 2004;91:1183-7.
Falch C, Stojadinovic A, von Weyhern CH, Protic M, Nissan A, Faries MB, et al. Anorectal malignant melanoma: extensive 45year review and proposal for a novel staging classification. J Am Coll Surg. 2013;217:324-35.
Heeney A, Mulsow J, Hyland J. Treatment and outcomes of anorectal melanoma. Surgeon. 2011;9:27-32.
Row D, Weiser MR. Anorectal melanoma. Clin Colon Rectal Surg. 2009;22:120-6.
Kanaan Z, Mulhall A, Mahid S, Torres ML, McCafferty M, McMasters KM, et al. A systemic review of prognosis and therapy of
anal malignant melanoma: a plea for more precise reporting of location and thickness. Am Surg. 2012;78:28-35.
Brady MS, Kavolius JP, Quan SH. Anorectal melanoma. A 64-year experience at Memorial Sloan-Kettering Cancer Center. Dis
Colon Rectum. 1995;38:146-51.
van Schaik PM, Ernst MF, Meijer HA, Bosscha K. Melanoma of the rectum: A rare entity. World J Gastroenterol 2008;14:1633-5.
Singer M, Mutch MG. Anal melanoma. Clin Colon Rectal Surg. 2006;19:78-87.
Slingluff CL Jr, Vollmer RT, Seigler HF. Anorectal melanoma: Clinical characteristics and results of surgical management in
twenty-four patients. Surgery 1990;107:1-9.
Liptrot S, Semeraro D, Ferguson A, Hurst N. Malignant melanoma of the rectum: A case report. J Med Case Rep 2009;3:9318.
DOI: 10.9790/0853-14931220
www.iosrjournals.org
19 | Page
Anorectal Melanoma: Radiologic-Pathologic Correlation
[13].
[14].
[15].
[16].
[17].
Stefanou A, Nalamati SP. Anorectal Melanoma. Clin Colon Rectal Surg. 2011;24:171-6.
Cagir B, Whiteford MH, Topham A, Rakinic J, Fry RD. Changing epidemiology of anorectal melanoma. Dis Colon Rectum
1999;42:1203-8.
Kim KW, Ha HK, Kim AY, Kim TK, Kim JS, Yu CS, et al. Primary malignant melanoma of the rectum: CT findings in eight
patients. Radiology 2004;232:181-6.
Matsuoka H, Nakamura A, Iwamoto K, Sugiyama M, Hachiya J, Atomi Y, et al. Anorectal malignant melanoma: Preoperative
usefulness of magnetic resonance imaging. J Gastroenterol 2005;40:836-42.
Carcoforo P, Raiji MT, Palini GM, Pedriali M, Maestroni U, Soliani G, et al. Primary anorectal melanoma: An update. J Cancer
2012;3:449-53.
DOI: 10.9790/0853-14931220
www.iosrjournals.org
20 | Page
Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationДокумент6 страницKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- New Drug Application HardДокумент37 страницNew Drug Application HardGANESH KUMAR JELLA100% (1)
- Swedish Medical Center Patient LetterДокумент2 страницыSwedish Medical Center Patient LetterMichael_Lee_RobertsОценок пока нет
- Human Rights and Dalits: Different Strands in The DiscourseДокумент5 страницHuman Rights and Dalits: Different Strands in The DiscourseInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Endometritis Unrelated To Pregnancy - UpToDateДокумент9 страницEndometritis Unrelated To Pregnancy - UpToDateLeoberto Batista Pereira SobrinhoОценок пока нет
- Medical Cert - EENTДокумент1 страницаMedical Cert - EENTHydie Lumadeo50% (2)
- Shallo El Hard I90 BДокумент2 страницыShallo El Hard I90 Belhard shalloОценок пока нет
- Community Herbal MedicineДокумент4 страницыCommunity Herbal MedicineMary Joyce Ariem100% (1)
- The Impact of Technologies On Society: A ReviewДокумент5 страницThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- NOSODESДокумент5 страницNOSODESnamkay_tenzynОценок пока нет
- Sujok Therapy FAQДокумент9 страницSujok Therapy FAQProbodh1100% (5)
- Presented by Animesh Amal: Brand Plan On Salbutamol + Ambroxol + GuaifenesinДокумент36 страницPresented by Animesh Amal: Brand Plan On Salbutamol + Ambroxol + GuaifenesinAnonymous 75aETJ8OОценок пока нет
- NABH 5 STD April 2020Документ120 страницNABH 5 STD April 2020kapil100% (7)
- Assessment of The Implementation of Federal Character in Nigeria.Документ5 страницAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Оценок пока нет
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweДокумент5 страниц"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityДокумент5 страницAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanДокумент7 страницSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Оценок пока нет
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionДокумент6 страницThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehДокумент4 страницыInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Оценок пока нет
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Документ15 страницA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Оценок пока нет
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeДокумент7 страницA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesДокумент7 страницComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Оценок пока нет
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyДокумент14 страницAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysДокумент5 страницEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsДокумент5 страницRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshДокумент7 страницTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Importance of Mass Media in Communicating Health Messages: An AnalysisДокумент6 страницImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Оценок пока нет
- The Lute Against Doping in SportДокумент5 страницThe Lute Against Doping in SportInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesДокумент5 страницDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalОценок пока нет
- Beowulf: A Folktale and History of Anglo-Saxon Life and CivilizationДокумент3 страницыBeowulf: A Folktale and History of Anglo-Saxon Life and CivilizationInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Transforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweДокумент9 страницTransforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Classical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahДокумент9 страницClassical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Role of Madarsa Education in Empowerment of Muslims in IndiaДокумент6 страницRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- An Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsДокумент6 страницAn Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Women Empowerment Through Open and Distance Learning in ZimbabweДокумент8 страницWomen Empowerment Through Open and Distance Learning in ZimbabweInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Motivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweДокумент8 страницMotivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Substance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaДокумент11 страницSubstance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Micro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaДокумент3 страницыMicro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Design Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextДокумент6 страницDesign Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextInternational Organization of Scientific Research (IOSR)Оценок пока нет
- A Study On The Television Programmes Popularity Among Chennai Urban WomenДокумент7 страницA Study On The Television Programmes Popularity Among Chennai Urban WomenInternational Organization of Scientific Research (IOSR)Оценок пока нет
- Rundown 2nd Annual Plastic Surgery in Daily PracticeДокумент2 страницыRundown 2nd Annual Plastic Surgery in Daily PracticeIzar AzwarОценок пока нет
- Update On Prenatal Diagnosis and Fetal Surgery ForДокумент15 страницUpdate On Prenatal Diagnosis and Fetal Surgery ForJULIETH ANDREA RUIZ PRIETOОценок пока нет
- Continuing Nursing Education: Importance of Lifelong LearningДокумент6 страницContinuing Nursing Education: Importance of Lifelong LearningDebashrita MisraОценок пока нет
- COVID-19 Environmental Health and Safety PlanДокумент23 страницыCOVID-19 Environmental Health and Safety PlanolaogunОценок пока нет
- Awareness Posters On Small Millets-English: Muniappan, KarthikeyanДокумент17 страницAwareness Posters On Small Millets-English: Muniappan, KarthikeyanSan ThoshОценок пока нет
- Ca BookДокумент80 страницCa BookSteivy Umaming TiwakenОценок пока нет
- Tarsal Tunnel SyndromeДокумент2 страницыTarsal Tunnel SyndromeMuhammad Amri KautsarОценок пока нет
- Module 1-Week 1-4 - Diet and HealthДокумент31 страницаModule 1-Week 1-4 - Diet and HealthAsteria RafalloОценок пока нет
- Department of Education: Republic of The PhilippinesДокумент3 страницыDepartment of Education: Republic of The PhilippinesRosalie Navales LegaspiОценок пока нет
- 14 Central Quadrant TechniqueДокумент10 страниц14 Central Quadrant TechniquemaytorenacgerОценок пока нет
- Henner PassДокумент1 страницаHenner PassFaez Al-AniОценок пока нет
- Placenta PreviaДокумент33 страницыPlacenta PreviamidoОценок пока нет
- Tugas Bahasa Inggris: Dosen Pengampu: Alfian Yoga Prananta, S.S, M. HumДокумент4 страницыTugas Bahasa Inggris: Dosen Pengampu: Alfian Yoga Prananta, S.S, M. HumDini AprilliyaniОценок пока нет
- Genetic Engineering MindmapДокумент1 страницаGenetic Engineering Mindmapgihan1mohamed1ahmedОценок пока нет
- Migmar Tsering (Mike) S ResumeДокумент3 страницыMigmar Tsering (Mike) S Resumeapi-284044370Оценок пока нет
- Fina Violita Christi-PaperДокумент5 страницFina Violita Christi-PaperFina ViolitaОценок пока нет
- Final Oral Health Resource May 2011 Web Version PDFДокумент137 страницFinal Oral Health Resource May 2011 Web Version PDFvyaa primasariОценок пока нет
- O Pt's Do NOT Move Gradually Through The Phases-Pt's Eb and Flow-Much More FluidДокумент4 страницыO Pt's Do NOT Move Gradually Through The Phases-Pt's Eb and Flow-Much More FluidKaitlyn ProbascoОценок пока нет
- 2028 Ajcc Melanoma and BeyondДокумент6 страниц2028 Ajcc Melanoma and BeyondDaniel Atl Lopez FabilaОценок пока нет
- Hypertension: Facts, Causes, Prevention and TreatmentДокумент18 страницHypertension: Facts, Causes, Prevention and TreatmentasepОценок пока нет