Вам также может понравиться
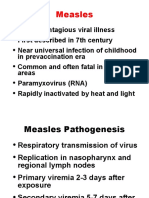
- MeaslesДокумент48 страницMeaslestiff-toff100% (1)
- Femtosecond Laser in Refractive and Cataract SurgeriesДокумент8 страницFemtosecond Laser in Refractive and Cataract Surgeriestiff-toffОценок пока нет
- MeningitisДокумент34 страницыMeningitistiff-toffОценок пока нет
- HaidДокумент6 страницHaidtiff-toffОценок пока нет
- Evaluation of Early Results of Quick-Chop Phacoemulsification in The Patients With High Myopic CataractДокумент4 страницыEvaluation of Early Results of Quick-Chop Phacoemulsification in The Patients With High Myopic Cataracttiff-toffОценок пока нет
- Long-Term Effects of Therapy With Ranibizumab On Diabetic Retinopathy Severity and Baseline Risk Factors For Worsening RetinopathyДокумент8 страницLong-Term Effects of Therapy With Ranibizumab On Diabetic Retinopathy Severity and Baseline Risk Factors For Worsening Retinopathytiff-toffОценок пока нет
- Anamnesis: (Recollection, A Patient Case History)Документ13 страницAnamnesis: (Recollection, A Patient Case History)AlbertoKosasihОценок пока нет
- WatermarkedAt A Glance 2016Документ8 страницWatermarkedAt A Glance 2016Sesilia Sri Yanti GaddyОценок пока нет
- Vital Signs and Temperature Measurements in PediatricsДокумент89 страницVital Signs and Temperature Measurements in Pediatricstiff-toffОценок пока нет
- Jurding CatarakДокумент8 страницJurding CatarakegyОценок пока нет
- Melani - Clinical Analysis of Risk Factors Contributing To Recurrence of Pterygium After Excision and Graft SurgeryДокумент6 страницMelani - Clinical Analysis of Risk Factors Contributing To Recurrence of Pterygium After Excision and Graft Surgerytiff-toffОценок пока нет
- Jurding MataДокумент4 страницыJurding Matatiff-toffОценок пока нет
- Long Term Results of No-Alcohol Laser Epithelial Keratomileusis and Photorefractive Keratectomy For MyopiaДокумент6 страницLong Term Results of No-Alcohol Laser Epithelial Keratomileusis and Photorefractive Keratectomy For Myopiatiff-toffОценок пока нет
- Cost-Effectiveness of Femtosecond Cost-Effectiveness of Femtosecond Laser-Assisted Cataract Surgery Versus Phacoemulsification Cataract SurgeryДокумент7 страницCost-Effectiveness of Femtosecond Cost-Effectiveness of Femtosecond Laser-Assisted Cataract Surgery Versus Phacoemulsification Cataract Surgerytiff-toffОценок пока нет
- Evaluation of Temporal Association Between Vaccinations and Retinal Hemorrhage in ChildrenДокумент5 страницEvaluation of Temporal Association Between Vaccinations and Retinal Hemorrhage in Childrentiff-toffОценок пока нет
- Association Between Metabolic Syndrome and Age-Related CataractДокумент8 страницAssociation Between Metabolic Syndrome and Age-Related Cataracttiff-toffОценок пока нет
- NICE Fever GuideДокумент38 страницNICE Fever Guidedante_chungaОценок пока нет
- Journal Article 16 246Документ8 страницJournal Article 16 246tiff-toffОценок пока нет
- PHD Buchmann TextДокумент223 страницыPHD Buchmann TextRidski D. MiruОценок пока нет
- UtiДокумент4 страницыUtitiff-toffОценок пока нет
- Advanced Cardiac Life Support PDFДокумент9 страницAdvanced Cardiac Life Support PDFYulias YoweiОценок пока нет
- Cardiovascular Emergencies ReviewДокумент78 страницCardiovascular Emergencies Reviewtiff-toffОценок пока нет
- HaidДокумент6 страницHaidtiff-toffОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Chapter 19 - Conditions Existing Before ConceptionДокумент6 страницChapter 19 - Conditions Existing Before ConceptionEunice CortésОценок пока нет
- Ent Practical Examinations Slides For StudyДокумент31 страницаEnt Practical Examinations Slides For StudyMuhdZaeedОценок пока нет
- Health Talk On Breast Self Examination-1Документ13 страницHealth Talk On Breast Self Examination-1priyanka50% (4)
- Hospital Pekan PresentationДокумент25 страницHospital Pekan PresentationImtiazОценок пока нет
- Presentation Otitis ExternaДокумент24 страницыPresentation Otitis ExternaRichard GunawanОценок пока нет
- Msds ODEXДокумент2 страницыMsds ODEXDevi ChintyaОценок пока нет
- Textbook of Obstetrics & GynecologyДокумент37 страницTextbook of Obstetrics & Gynecologysanjivdas0% (1)
- Joni DialogДокумент3 страницыJoni DialogJoni TriliwijayaОценок пока нет
- 2017 05 GC Pocket CardДокумент2 страницы2017 05 GC Pocket Cardapi-312241089Оценок пока нет
- Clinical Practice Guidelines 11-18Документ20 страницClinical Practice Guidelines 11-18Feroz RaZa SoomrOoОценок пока нет
- Guidance Notes On Use of Uterotonics During LaborДокумент28 страницGuidance Notes On Use of Uterotonics During LaborKinjal VasavaОценок пока нет
- Your Travel Insurance Policy: Reference Number: Insurefor/EA/2009 09IST, 09ISA & 09ISEДокумент12 страницYour Travel Insurance Policy: Reference Number: Insurefor/EA/2009 09IST, 09ISA & 09ISEOmar DahouОценок пока нет
- Postpartum HemorrhageДокумент16 страницPostpartum HemorrhageLuayon FrancisОценок пока нет
- Mindanao Medical Foundation College: P. Villanueva ST., Agdao, Davao City Tel. No. (082) 221-6225Документ5 страницMindanao Medical Foundation College: P. Villanueva ST., Agdao, Davao City Tel. No. (082) 221-6225Miles Asia DieroОценок пока нет
- Acupuncture Boosts IVF Success RatesДокумент10 страницAcupuncture Boosts IVF Success RatesWolfgang Rb100% (1)
- Anterior Compartment of Arm & Cubital FossaДокумент24 страницыAnterior Compartment of Arm & Cubital FossaSky StoneОценок пока нет
- 06-Seminars in Fetal DevelopmentДокумент75 страниц06-Seminars in Fetal DevelopmentGanesh Subramanian MohanОценок пока нет
- Skin Cancer TBL 2 2f3Документ19 страницSkin Cancer TBL 2 2f3api-356476029Оценок пока нет
- Health Check-Up BriefДокумент5 страницHealth Check-Up Briefજીસીએસ હોસ્પિટલОценок пока нет
- Coock Consommable PDFДокумент110 страницCoock Consommable PDFsaidbenmokhtar3960Оценок пока нет
- Palatal Plane MeasurementДокумент6 страницPalatal Plane MeasurementRavi ChandraОценок пока нет
- Rogelio Nogales Vs Capitol Medical CenterДокумент8 страницRogelio Nogales Vs Capitol Medical CenterMaius GaerlanОценок пока нет
- Analgesia en ObstetriciaДокумент21 страницаAnalgesia en ObstetriciaSERGIO VERGEL MANTILLAОценок пока нет
- ASEAN Mutual Recognition Arrangement For Indonesian Nurses: Is It A Promise?Документ4 страницыASEAN Mutual Recognition Arrangement For Indonesian Nurses: Is It A Promise?Krisha JacobОценок пока нет
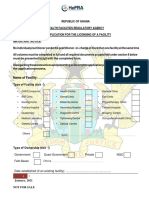
- HeFRA APPLICATION FORM V7.0 FREEДокумент10 страницHeFRA APPLICATION FORM V7.0 FREEMichael BusiaОценок пока нет
- Topic 5 Nursing Care of The High-Risk Post-Partal ClientsДокумент51 страницаTopic 5 Nursing Care of The High-Risk Post-Partal ClientsMarissa A AquinoОценок пока нет
- Skilled Occupation List (SOL) : Schedule 1: Australian Government Department of Immigration and CitizenshipДокумент6 страницSkilled Occupation List (SOL) : Schedule 1: Australian Government Department of Immigration and Citizenshipmd abОценок пока нет
- HERICOДокумент3 страницыHERICOBryant AndunganОценок пока нет
- DR ActivityДокумент2 страницыDR ActivityVia Teresa AtienzaОценок пока нет
- Exp 3Документ7 страницExp 3Chan Wei QuanОценок пока нет