Вам также может понравиться
- Laboratory Values Cheat Sheet NCLEX - US Legal Size (8.5 x14 ) Paper (Caribbean Nurses of Puerto Rico and Latin America)Документ2 страницыLaboratory Values Cheat Sheet NCLEX - US Legal Size (8.5 x14 ) Paper (Caribbean Nurses of Puerto Rico and Latin America)ChristineBiankiiОценок пока нет
- Laboratory Values Cheat Sheet NCLEX - US Legal Size (8.5 x14 ) Paper (Caribbean Nurses of Puerto Rico and Latin America)Документ2 страницыLaboratory Values Cheat Sheet NCLEX - US Legal Size (8.5 x14 ) Paper (Caribbean Nurses of Puerto Rico and Latin America)ChristineBiankiiОценок пока нет
- Laboratory Values Cheat Sheet NCLEX - US Legal Size (8.5 x14 ) Paper (Caribbean Nurses of Puerto Rico and Latin America)Документ2 страницыLaboratory Values Cheat Sheet NCLEX - US Legal Size (8.5 x14 ) Paper (Caribbean Nurses of Puerto Rico and Latin America)ChristineBiankiiОценок пока нет
- Dosing Titration ScheduleДокумент1 страницаDosing Titration ScheduleKumar BhaiОценок пока нет
- 2015 06 Viewbook WebДокумент11 страниц2015 06 Viewbook WebKumar BhaiОценок пока нет
- Crushing and Liquid ARV FormulationsДокумент18 страницCrushing and Liquid ARV FormulationsKumar BhaiОценок пока нет
- Penicillin PDFДокумент1 страницаPenicillin PDFKumar Bhai0% (1)
- Penicillin PDFДокумент1 страницаPenicillin PDFKumar Bhai0% (1)
- 7 11Документ6 страниц7 11Uswatun MaulidiyahОценок пока нет
- Penicillin PDFДокумент1 страницаPenicillin PDFKumar Bhai0% (1)
- Steroid Potency ChartДокумент1 страницаSteroid Potency ChartKumar Bhai100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Transfer of Genetic InformationДокумент13 страницTransfer of Genetic InformationjaneОценок пока нет
- BREASTFEEDING EDUCATIONДокумент10 страницBREASTFEEDING EDUCATIONJm Tolentino100% (1)
- DiarrheaДокумент2 страницыDiarrheaJonah reiОценок пока нет
- Quiz On School Health NursingДокумент7 страницQuiz On School Health Nursingchoobi0% (2)
- Word Analogy Word ClassificationДокумент4 страницыWord Analogy Word Classificationk.ramakrishnaОценок пока нет
- Microbes in Household Products Part I PDFДокумент33 страницыMicrobes in Household Products Part I PDFAkash NaskarОценок пока нет
- Yutaka Oki M D Auth Lewis S Blevins JR M D Eds Cushing 2002Документ347 страницYutaka Oki M D Auth Lewis S Blevins JR M D Eds Cushing 2002Jhoan DanielОценок пока нет
- 17.4.01B AOAC Official Method 996.10 Escherichia Coli O157:H7 in Selected FoodsДокумент3 страницы17.4.01B AOAC Official Method 996.10 Escherichia Coli O157:H7 in Selected FoodsJaimeEstradaCОценок пока нет
- Influenza Vaccination Case StudyДокумент2 страницыInfluenza Vaccination Case StudySara Lynn LeSage75% (4)
- Department of Molecular Biology. Covid 19 Test Name Result Unit Bio. Ref. Range MethodДокумент2 страницыDepartment of Molecular Biology. Covid 19 Test Name Result Unit Bio. Ref. Range Methodvamsi krishnaОценок пока нет
- III BSC BT - 609 A - Core - Animal BiotechnologyДокумент19 страницIII BSC BT - 609 A - Core - Animal BiotechnologyRamesh BeniwalОценок пока нет
- DS - Aseptoman® Plus - Pif - en - 1711Документ2 страницыDS - Aseptoman® Plus - Pif - en - 1711Serbanica RazvanОценок пока нет
- SRL DigestДокумент186 страницSRL DigestD. GandhirajОценок пока нет
- Diffuse Midline Glioma: DR Tamajyoti GhoshДокумент53 страницыDiffuse Midline Glioma: DR Tamajyoti GhoshTamajyoti Ghosh100% (1)
- Cholestasis: View Full-Size ImageДокумент15 страницCholestasis: View Full-Size Imagearambakkam100% (2)
- Human Physiology ExamsДокумент198 страницHuman Physiology Examsdaw02250% (4)
- Learning Outcomes Genetic Variation and Change 2 5Документ2 страницыLearning Outcomes Genetic Variation and Change 2 5api-292477453Оценок пока нет
- Protein SynthesisДокумент2 страницыProtein SynthesisArlan AbraganОценок пока нет
- Genomic Imprinting Is An Epigenetic Phenomenon That Causes Genes To Be Expressed in A Parent-OfДокумент3 страницыGenomic Imprinting Is An Epigenetic Phenomenon That Causes Genes To Be Expressed in A Parent-OfRamy El-HadadОценок пока нет
- Jupeb 2019 Biology SyllabusДокумент20 страницJupeb 2019 Biology SyllabusAlexis RockelleОценок пока нет
- Chapter 9 GeneticsДокумент32 страницыChapter 9 GeneticsasdfОценок пока нет
- Understandings, Applications and Skills (This Is What You Maybe Assessed On)Документ10 страницUnderstandings, Applications and Skills (This Is What You Maybe Assessed On)beaОценок пока нет
- Molluscum Contagiosum An Update and Review of Prespectives Etiology, Diagnosis, and Treatment PDFДокумент9 страницMolluscum Contagiosum An Update and Review of Prespectives Etiology, Diagnosis, and Treatment PDFLaras KinasihОценок пока нет
- Name: Babafemi Bunmi Oluwatosin Reg No. VU-BNS-2001-0049 Course: Anatomy & Physiology 1 Topic: Leukemia (Blood Cancer)Документ7 страницName: Babafemi Bunmi Oluwatosin Reg No. VU-BNS-2001-0049 Course: Anatomy & Physiology 1 Topic: Leukemia (Blood Cancer)Bunmi OluwatosinОценок пока нет
- Chemical Messengers - 1Документ10 страницChemical Messengers - 1Ryan GosserОценок пока нет
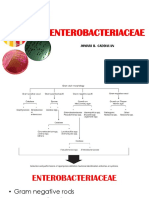
- EXO-Notes JBC ENTEROBACTERIACEAEДокумент70 страницEXO-Notes JBC ENTEROBACTERIACEAECha Tangan-PenolОценок пока нет
- Lymphoma in D&C-VetcvasДокумент127 страницLymphoma in D&C-VetcvasAnne DelefrateОценок пока нет
- Genetics Study Guide Answers 1Документ2 страницыGenetics Study Guide Answers 1KellyОценок пока нет
- MHC Class I and II Antigens Present Foreign Antigens to T CellsДокумент16 страницMHC Class I and II Antigens Present Foreign Antigens to T CellssharanОценок пока нет
- Complete Rate List 2019 Updated PDFДокумент17 страницComplete Rate List 2019 Updated PDFManal Latif100% (2)