Вам также может понравиться
- Antipsychotics - FactsheetДокумент12 страницAntipsychotics - FactsheetColonОценок пока нет
- FA 2016 Step 1 - Reference ValuesДокумент2 страницыFA 2016 Step 1 - Reference ValuesJUSASBОценок пока нет
- Toronto Notes Nephrology 2015 38Документ1 страницаToronto Notes Nephrology 2015 38JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 33Документ1 страницаToronto Notes Nephrology 2015 33JUSASBОценок пока нет
- COMLEX Normal Adult Laboratory ValuesДокумент5 страницCOMLEX Normal Adult Laboratory ValuesJUSASBОценок пока нет
- Antipsychotics Factsheet pg2Документ1 страницаAntipsychotics Factsheet pg2JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 37Документ1 страницаToronto Notes Nephrology 2015 37JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 39Документ1 страницаToronto Notes Nephrology 2015 39JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 27Документ1 страницаToronto Notes Nephrology 2015 27JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 30Документ1 страницаToronto Notes Nephrology 2015 30JUSASBОценок пока нет
- References: NP40 Nephrology Landmark Nephrology Trials/References Essential Med Notes 2015Документ1 страницаReferences: NP40 Nephrology Landmark Nephrology Trials/References Essential Med Notes 2015JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 35Документ1 страницаToronto Notes Nephrology 2015 35JUSASB50% (2)
- Toronto Notes Nephrology 2015 36Документ1 страницаToronto Notes Nephrology 2015 36JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 28Документ1 страницаToronto Notes Nephrology 2015 28JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 24Документ1 страницаToronto Notes Nephrology 2015 24JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 34Документ1 страницаToronto Notes Nephrology 2015 34JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 31Документ1 страницаToronto Notes Nephrology 2015 31JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 5Документ1 страницаToronto Notes Nephrology 2015 5JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 17Документ1 страницаToronto Notes Nephrology 2015 17JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 26Документ1 страницаToronto Notes Nephrology 2015 26JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 29Документ1 страницаToronto Notes Nephrology 2015 29JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 32Документ1 страницаToronto Notes Nephrology 2015 32JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 23Документ1 страницаToronto Notes Nephrology 2015 23JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 20Документ1 страницаToronto Notes Nephrology 2015 20JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 25Документ1 страницаToronto Notes Nephrology 2015 25JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 18Документ1 страницаToronto Notes Nephrology 2015 18JUSASBОценок пока нет
- Toronto Notes Nephrology 2015 22Документ1 страницаToronto Notes Nephrology 2015 22JUSASB0% (1)
- Toronto Notes Nephrology 2015 15Документ1 страницаToronto Notes Nephrology 2015 15JUSASBОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Robert Harr's Clinical Chemistry Questions About ElectrolytesДокумент7 страницRobert Harr's Clinical Chemistry Questions About ElectrolytesDIEGO RAFAEL ESPIRITUОценок пока нет
- Management of Hyperkalaemia and HypokalaemiaДокумент21 страницаManagement of Hyperkalaemia and Hypokalaemiaferoza97Оценок пока нет
- Hyper Kale Mia Case ReviewДокумент4 страницыHyper Kale Mia Case ReviewSamina AhmadОценок пока нет
- Case Report - CahДокумент3 страницыCase Report - Cahbella satriawanОценок пока нет
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesДокумент44 страницыElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaОценок пока нет
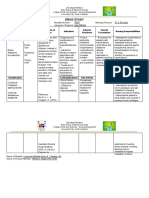
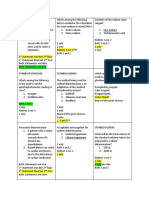
- Assessment Explanatio Nofthe Problem Objectives Nursing Intervention Rationale EvaluationДокумент3 страницыAssessment Explanatio Nofthe Problem Objectives Nursing Intervention Rationale EvaluationAziil LiizaОценок пока нет
- Patophysiology Oral Q 1Документ134 страницыPatophysiology Oral Q 1TijanaОценок пока нет
- Drug Study: Santiago, J. L. 243-D Dr. E. de Lunas Liver CirrhosisДокумент2 страницыDrug Study: Santiago, J. L. 243-D Dr. E. de Lunas Liver CirrhosisNathalia CabalseОценок пока нет
- KMMMMMMMMMMMMMMMMДокумент14 страницKMMMMMMMMMMMMMMMMJerecel Gapi VigoОценок пока нет
- Downer Cow SyndromeДокумент20 страницDowner Cow SyndromeRizka MuelldoОценок пока нет
- FENOTEROLДокумент20 страницFENOTEROLCristian ColosoОценок пока нет
- Surgery Made Easy V1 PDFДокумент125 страницSurgery Made Easy V1 PDFطلال العمريОценок пока нет
- Hyperkalemia and HypokalemiaДокумент37 страницHyperkalemia and HypokalemiaDiena AshlihatiОценок пока нет
- Mr. William's Case StudyДокумент2 страницыMr. William's Case StudyChelsea AquinoОценок пока нет
- Fluid and Electrolytes Study GuideДокумент16 страницFluid and Electrolytes Study GuideDianaNursing96% (28)
- Impact of Reduced Potassium Nitrate Concentrations in Nutrient Solution On The Growth, Yield and Fruit Quality of Melon in Hydroponics.Документ11 страницImpact of Reduced Potassium Nitrate Concentrations in Nutrient Solution On The Growth, Yield and Fruit Quality of Melon in Hydroponics.Riz Jomaica ArenasОценок пока нет
- Potassiumchlorideoral PDFДокумент2 страницыPotassiumchlorideoral PDFShaira TanОценок пока нет
- Seminar On Fluid-and-Electrolyte-ImbalanceДокумент35 страницSeminar On Fluid-and-Electrolyte-Imbalancemohamad dildarОценок пока нет
- Fluids & Electrolyte NewДокумент154 страницыFluids & Electrolyte NewMaria Visitacion100% (2)
- Lactated Ringer'sДокумент10 страницLactated Ringer'sJeannette Richelle DacilloОценок пока нет
- Fundamental of Nursing-NleДокумент8 страницFundamental of Nursing-NleJade DigoОценок пока нет
- PCP in A Box - Module 2Документ49 страницPCP in A Box - Module 2shaheershayanqaziОценок пока нет
- Name: Ribca Mariam CMS:17961 Subject: Biochemistry and Genetics Submitted To: Sir Mobin MustafaДокумент20 страницName: Ribca Mariam CMS:17961 Subject: Biochemistry and Genetics Submitted To: Sir Mobin MustafaRibca MariamОценок пока нет
- Acute Renal FailureДокумент35 страницAcute Renal FailureKaelyn Bello Giray100% (1)
- IVF SolutionsДокумент22 страницыIVF SolutionsFatima CorpuzОценок пока нет
- Cc2lab Sodium Potassium Quiz WT RevДокумент13 страницCc2lab Sodium Potassium Quiz WT RevJHON JORIES VISMONTEОценок пока нет
- NCA2 PosttestsДокумент20 страницNCA2 PosttestsCzarena Ysabelle PayotОценок пока нет
- Drug Dosage Mechanism of Action Specific Indicatio N Contraindicat ION Adverse Effect Nursing PrecautionДокумент14 страницDrug Dosage Mechanism of Action Specific Indicatio N Contraindicat ION Adverse Effect Nursing PrecautionIzabela UyОценок пока нет
- Cardiotonic DrugsДокумент67 страницCardiotonic DrugsLady Mae Ramos100% (1)
- SodiumДокумент4 страницыSodiumsandeep4485Оценок пока нет