Вам также может понравиться
- Emergency War Surgery GuideДокумент480 страницEmergency War Surgery GuidePathfinder!100% (3)
- Pararescue Medication and Procedure Handbook-1Документ137 страницPararescue Medication and Procedure Handbook-1Charles Harris100% (1)
- @anesthesia Books 2017 EssentialsДокумент346 страниц@anesthesia Books 2017 EssentialsAnonymous EQnqbCTОценок пока нет
- Jurnal Flail Chest.Документ6 страницJurnal Flail Chest.Dessy Christiani Part IIОценок пока нет
- Maxillofacial Trauma and Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Документ24 страницыMaxillofacial Trauma and Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghОценок пока нет
- Obstetrics OverviewДокумент91 страницаObstetrics OverviewAbi TudОценок пока нет
- Nelson Pediatrics Review (MCQS) 17edДокумент631 страницаNelson Pediatrics Review (MCQS) 17edGabrielle Maycock75% (8)
- Manual of Definitive Surgical Trauma Care PDFДокумент238 страницManual of Definitive Surgical Trauma Care PDFUmer Khan100% (1)
- Nursing Diagnosis For CataractДокумент3 страницыNursing Diagnosis For CataractZainul HazwanОценок пока нет
- Scope of Forensic RadiologyДокумент15 страницScope of Forensic RadiologyZiniaKhanОценок пока нет
- Hypovolemic ShockДокумент8 страницHypovolemic ShockLyka Flores100% (1)
- AtlsДокумент2 страницыAtlsAlexandros Megas100% (2)
- Soal ATLSДокумент12 страницSoal ATLSarditya galaxy100% (1)
- Thoracic Trauma - Navy - PSPD 2021Документ45 страницThoracic Trauma - Navy - PSPD 2021Naavy LaksmonoОценок пока нет
- Timing of Surgery For Aneurysmal Subarachnoid Hemorrhage - A Systematic Review and Meta-AnalysisДокумент9 страницTiming of Surgery For Aneurysmal Subarachnoid Hemorrhage - A Systematic Review and Meta-AnalysisJulieta PereyraОценок пока нет
- Efficacy and Safety of Restrictive Blood TransfusiДокумент4 страницыEfficacy and Safety of Restrictive Blood TransfusiJustin Jay Dar IОценок пока нет
- Subclinical Hypoperfusion in Trauma Patients and Its Influence On Surgical Fracture Fixation: Systematic Review and Meta-AnalysisДокумент9 страницSubclinical Hypoperfusion in Trauma Patients and Its Influence On Surgical Fracture Fixation: Systematic Review and Meta-AnalysisMateoZuluagaGomezОценок пока нет
- Saar 2016Документ7 страницSaar 2016iinmsОценок пока нет
- Ref 6Документ9 страницRef 6riskaicungОценок пока нет
- Early Surgery Confers One-Year Mortality Benefit in Hip-Fracture PatientsДокумент12 страницEarly Surgery Confers One-Year Mortality Benefit in Hip-Fracture PatientsMartin MontesОценок пока нет
- 1 s2.0 S1053077022009168 MainДокумент8 страниц1 s2.0 S1053077022009168 MainOttofianus Alvedo Hewick KalangiОценок пока нет
- Original Article: The Weekend Effect: Does Time of Admission Impact Management and Outcomes of Small Bowel Obstruction?Документ5 страницOriginal Article: The Weekend Effect: Does Time of Admission Impact Management and Outcomes of Small Bowel Obstruction?DeVisShoppОценок пока нет
- IPHMILitRev V5.2Документ5 страницIPHMILitRev V5.2miguel angel camachoОценок пока нет
- Ivac 176Документ5 страницIvac 176Issa AbuzeidОценок пока нет
- The Influence of Timing of Surgical Decompression For Acute Spinal Cord Injury - A Pooled Analysis of Individual Patient DataДокумент10 страницThe Influence of Timing of Surgical Decompression For Acute Spinal Cord Injury - A Pooled Analysis of Individual Patient DataballroomchinaОценок пока нет
- RadioДокумент4 страницыRadiomuhammad robyОценок пока нет
- Critical (17-24)Документ15 страницCritical (17-24)kololll lllknОценок пока нет
- Surgical Trial in Lobar Intracerebral Haemorrhage Protocol: Version 1.3 / 10 August 2006Документ23 страницыSurgical Trial in Lobar Intracerebral Haemorrhage Protocol: Version 1.3 / 10 August 2006bodeadumitru9261100% (1)
- Luan2019 PDFДокумент12 страницLuan2019 PDFrifki irsyadОценок пока нет
- Preoperative Assessment of The Risk For Multiple Complications After SurgeryДокумент10 страницPreoperative Assessment of The Risk For Multiple Complications After SurgerylaisОценок пока нет
- Readmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsДокумент9 страницReadmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsbobОценок пока нет
- Effects of Timing of Appendectomy On The Risks of Perforation and Postoperative Complications of Acute AppendicitisДокумент9 страницEffects of Timing of Appendectomy On The Risks of Perforation and Postoperative Complications of Acute AppendicitisLydia EniithОценок пока нет
- Rcsann 2016 0048Документ6 страницRcsann 2016 0048fabian arassiОценок пока нет
- Nottingham Hip Fracture Score As A PredictorДокумент4 страницыNottingham Hip Fracture Score As A PredictorRENAULTОценок пока нет
- Coach 2023Документ11 страницCoach 2023Guilherme CarelliОценок пока нет
- Journal of Clinical AnesthesiaДокумент6 страницJournal of Clinical AnesthesiaGabriela Estrada RenteríaОценок пока нет
- Bed Angels On PainДокумент12 страницBed Angels On PainNiken AninditaОценок пока нет
- Jurnal EBM WBWMДокумент10 страницJurnal EBM WBWMUliza Nur AiniОценок пока нет
- Skoretz 2014Документ8 страницSkoretz 2014Gonzalo FragaОценок пока нет
- Prehospital Thrombolysis: It S All About Time: February 2012Документ23 страницыPrehospital Thrombolysis: It S All About Time: February 2012deo rizkyОценок пока нет
- Journal Cardiac ArrestДокумент6 страницJournal Cardiac ArrestDavid Fransiskus SimarmataОценок пока нет
- JOT - 2015 - Childs - Obesity Is Associated W More Complicatiosn and Longer Hospital Stays After Ortho TraumaДокумент6 страницJOT - 2015 - Childs - Obesity Is Associated W More Complicatiosn and Longer Hospital Stays After Ortho TraumaJacob DoughertyОценок пока нет
- Retrospective Review of Necrotizing Fasciitis in Hong Kong HospitalДокумент32 страницыRetrospective Review of Necrotizing Fasciitis in Hong Kong HospitalHam FGОценок пока нет
- Anesthesia Needs Large International Clinical Trials: Mcmaster University, Ontario, CanadaДокумент4 страницыAnesthesia Needs Large International Clinical Trials: Mcmaster University, Ontario, Canadaserena7205Оценок пока нет
- Factors Associated With Short-Term Mortality After Surgical Oncologic EmergenciesДокумент12 страницFactors Associated With Short-Term Mortality After Surgical Oncologic EmergenciesErinda SafitriОценок пока нет
- Articulo 1Документ8 страницArticulo 1Julio Cosme CastorenaОценок пока нет
- Severe Head Injury Clinical PathwayДокумент7 страницSevere Head Injury Clinical PathwaytheodoruskevinОценок пока нет
- The Influence of Perioperative Care and Treatment On The 4-Month Outcome in Elderly Patients With Hip FractureДокумент12 страницThe Influence of Perioperative Care and Treatment On The 4-Month Outcome in Elderly Patients With Hip FractureResti LovitaОценок пока нет
- Sedaghat-2015-Impact of Day of Week On OutcomeДокумент5 страницSedaghat-2015-Impact of Day of Week On OutcomeLuca BertolacciniОценок пока нет
- 586 2003 Article 493Документ12 страниц586 2003 Article 493abdurrahmanОценок пока нет
- Factors Related To Delayed Extubation in Cervical SpineДокумент6 страницFactors Related To Delayed Extubation in Cervical SpineAhmad Rizal MОценок пока нет
- 28nnadi EtalДокумент4 страницы28nnadi EtaleditorijmrhsОценок пока нет
- Endovascular Stentgraft Placement in Aortic Dissection A MetaanalysisДокумент10 страницEndovascular Stentgraft Placement in Aortic Dissection A MetaanalysisCiubuc AndrianОценок пока нет
- 1 StrokeДокумент10 страниц1 StrokeRekyan ListyaningsihОценок пока нет
- Arthroplasty TodayДокумент4 страницыArthroplasty TodayCristina SavaОценок пока нет
- Who Should Be Operated When Presenting With A Ruptured Abdominal AorticДокумент18 страницWho Should Be Operated When Presenting With A Ruptured Abdominal AorticVlad NeagoeОценок пока нет
- Diameter 1Документ6 страницDiameter 1Nouchan NoupОценок пока нет
- Journal of Trauma Management & OutcomesДокумент6 страницJournal of Trauma Management & OutcomesNotariana Kusuma AОценок пока нет
- Infection As An Independent Risk Factor For Mortality in The Surgical Intensive Care UnitДокумент6 страницInfection As An Independent Risk Factor For Mortality in The Surgical Intensive Care UnitTito Ahmad RizkiawanОценок пока нет
- 1 s2.0 S0883944118301850 MainДокумент7 страниц1 s2.0 S0883944118301850 MainWAI PAN WONGОценок пока нет
- Delayed Seizures After Intracerebral HaemorrhageДокумент12 страницDelayed Seizures After Intracerebral HaemorrhageTaufik 81Оценок пока нет
- Short and Long-Term Outcomes After Surgical Procedures Lasting For More Than Six HoursДокумент8 страницShort and Long-Term Outcomes After Surgical Procedures Lasting For More Than Six HoursDickyОценок пока нет
- Is It Safe To Discharge Intussusception Patients After Successful Hydrostatic Reduction?Документ5 страницIs It Safe To Discharge Intussusception Patients After Successful Hydrostatic Reduction?DaGiTrVel'zОценок пока нет
- Anesthesia Technique and Mortality 2016Документ8 страницAnesthesia Technique and Mortality 2016John Portales ArmasОценок пока нет
- Assessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryДокумент8 страницAssessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryIJAR JOURNALОценок пока нет
- 0507 InsulinprotocolДокумент7 страниц0507 InsulinprotocolRianda PuspitaОценок пока нет
- Neurosurgery UpdateДокумент30 страницNeurosurgery UpdateGustavo Xavier Ayarza PulidoОценок пока нет
- Fast Track CaderaДокумент6 страницFast Track CaderaJulianОценок пока нет
- Clinical Approach For The Pneumomediastinum After Blunt Chest TraumaДокумент7 страницClinical Approach For The Pneumomediastinum After Blunt Chest TraumaIdham Adyasa Manggala PutraОценок пока нет
- Mortality After Esophagectomy: Analysis of Individual Complications and Their Association With MortalityДокумент7 страницMortality After Esophagectomy: Analysis of Individual Complications and Their Association With MortalityMaria PalОценок пока нет
- Achieving Sustainability in Reducing Unplanned Extubations in PICUДокумент7 страницAchieving Sustainability in Reducing Unplanned Extubations in PICUKevin Bazán TorrealvaОценок пока нет
- Use of Ketorolac Is Associated With Decreased Pneumonia Following Rib FracturesДокумент7 страницUse of Ketorolac Is Associated With Decreased Pneumonia Following Rib Fracturesracut_khansatraОценок пока нет
- Case Studies of Postoperative Complications after Digestive SurgeryОт EverandCase Studies of Postoperative Complications after Digestive SurgeryОценок пока нет
- Glucose Counterregulatory Responses To HypoglycemiaДокумент19 страницGlucose Counterregulatory Responses To HypoglycemiaZeptAlanОценок пока нет
- Arterial Vascularization of The Pineal Gland: Original PaperДокумент7 страницArterial Vascularization of The Pineal Gland: Original PaperZeptAlanОценок пока нет
- Turkish Neurosurg 13 - Surgical Management of TISDHДокумент6 страницTurkish Neurosurg 13 - Surgical Management of TISDHZeptAlanОценок пока нет
- Acta Neurochir 14 - MiniCraniotomia As Primary Surgical Intervention For The Treatment of CSDHДокумент7 страницActa Neurochir 14 - MiniCraniotomia As Primary Surgical Intervention For The Treatment of CSDHZeptAlanОценок пока нет
- J Clin NeuroSc 14 - Time Interval To Surgery and Outcomes Following The Surgical Treatment of Actue Traumatic Subdural HematomaДокумент5 страницJ Clin NeuroSc 14 - Time Interval To Surgery and Outcomes Following The Surgical Treatment of Actue Traumatic Subdural HematomaZeptAlanОценок пока нет
- 2007 Weaning From Mechanical VentilationДокумент24 страницы2007 Weaning From Mechanical VentilationZeptAlanОценок пока нет
- J Neurosurg 14 - Chronic Subdural Hematoma - A Systematic Review and Meta-Analysis of Surgical ProceduresДокумент9 страницJ Neurosurg 14 - Chronic Subdural Hematoma - A Systematic Review and Meta-Analysis of Surgical ProceduresZeptAlanОценок пока нет
- Art:10 1023/A:1012790213818Документ13 страницArt:10 1023/A:1012790213818ZeptAlanОценок пока нет
- 2007 Weaning From Mechanical VentilationДокумент24 страницы2007 Weaning From Mechanical VentilationZeptAlanОценок пока нет
- 1 Early Management of Trauma Patient in The HospitalДокумент23 страницы1 Early Management of Trauma Patient in The HospitalkgnmatinОценок пока нет
- Pediatric Disaster PreparednessДокумент196 страницPediatric Disaster Preparednessccbrown7100% (1)
- Trevor Tice Medical Examiners ReportДокумент8 страницTrevor Tice Medical Examiners ReportBayAreaNewsGroupОценок пока нет
- Stop The Bleed Booklet FinalДокумент16 страницStop The Bleed Booklet FinalUrsula MalauОценок пока нет
- ErgonomicsДокумент66 страницErgonomicsAshmit Anand0% (1)
- Anesthesia For Patients With Acute Traumatic Brain InjuryДокумент51 страницаAnesthesia For Patients With Acute Traumatic Brain InjurymandeepОценок пока нет
- Crash 2Документ12 страницCrash 2Fredy OrtizОценок пока нет
- Letter To Members of The SenateДокумент1 страницаLetter To Members of The SenateEduardo SotoОценок пока нет
- Emtiaz Guide in SurgeryДокумент25 страницEmtiaz Guide in SurgeryMohamed AwadОценок пока нет
- Jadwal Atls Online 12 November 2022, JKTДокумент4 страницыJadwal Atls Online 12 November 2022, JKTJeremyBetaОценок пока нет
- SGD 6 LBM 4 FractureДокумент4 страницыSGD 6 LBM 4 FractureMonica Wyona LorensiaОценок пока нет
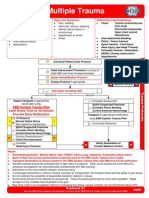
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationДокумент1 страницаMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonОценок пока нет
- Prematurity, Dysmaturity, Postmaturity PDFДокумент8 страницPrematurity, Dysmaturity, Postmaturity PDFMuhammad YaminОценок пока нет
- AAST - WSES Guidelines On Diagnosis and Management of Peripheral Vascular InjuriesДокумент66 страницAAST - WSES Guidelines On Diagnosis and Management of Peripheral Vascular InjuriesSandra Milena Sepùlveda Bastilla100% (1)
- Injury Severity ScoresДокумент32 страницыInjury Severity ScoresscribdnillyОценок пока нет
- Assignment On Disaster Management: School of Management Studies, Punjabi University, PatialaДокумент13 страницAssignment On Disaster Management: School of Management Studies, Punjabi University, PatialaKawalpreet Singh MakkarОценок пока нет
- Emergency Management of The Patient With Severe Burns in The Emergency UnitДокумент9 страницEmergency Management of The Patient With Severe Burns in The Emergency UnitAnonymous LnWIBo1GОценок пока нет