Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Tacfit Survival - Bonus1 28 Days PrimalДокумент17 страницTacfit Survival - Bonus1 28 Days Primalimre100% (1)
- Micronutrients in Hair LossДокумент9 страницMicronutrients in Hair LossIkbal Adi SaputraОценок пока нет
- HowtogrowtallerДокумент30 страницHowtogrowtallerPhu TRANОценок пока нет
- Medical Nutrition Therapy For Hemodialysis PatientsДокумент24 страницыMedical Nutrition Therapy For Hemodialysis Patientsraquelt_65Оценок пока нет
- Latihan Penilaian Harian 3Документ2 страницыLatihan Penilaian Harian 3FEBRIAN RISQI FIRMANSYAHОценок пока нет
- Vitamins All AboutДокумент31 страницаVitamins All Aboutvu aneelaОценок пока нет
- Passmedicine MRCP Notes-NephrologyДокумент73 страницыPassmedicine MRCP Notes-Nephrologysalwabeshir542Оценок пока нет
- Vitamins & Minerals: Name: - DateДокумент1 страницаVitamins & Minerals: Name: - DateWiktoria StahlОценок пока нет
- Biochemical Assessment of Vitamin DДокумент24 страницыBiochemical Assessment of Vitamin DKarunya VkОценок пока нет
- Dietary Recommendations For Toddlers, Preschool, and School-Age Children - UpToDateДокумент39 страницDietary Recommendations For Toddlers, Preschool, and School-Age Children - UpToDateĐỗ Trần Giang SơnОценок пока нет
- Abstracts On NDDSДокумент55 страницAbstracts On NDDSprasanthiОценок пока нет
- Instruction: Read The Instructions Carefully and Answer Directly To The Test QuestionnaireДокумент6 страницInstruction: Read The Instructions Carefully and Answer Directly To The Test QuestionnaireMenoj SantuyoОценок пока нет
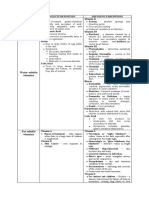
- Water Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin AДокумент3 страницыWater Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin ARoshin TejeroОценок пока нет
- CHEM216 Research 8Документ5 страницCHEM216 Research 8Theo Vito PradipaОценок пока нет
- Practice 1 m12 Đã G PДокумент22 страницыPractice 1 m12 Đã G PAnh ThưОценок пока нет
- Chapter 11 - Nutrition Through The Life Span: Pregnancy and LactationДокумент12 страницChapter 11 - Nutrition Through The Life Span: Pregnancy and LactationMario MagtakaОценок пока нет
- Southern Derbyshire Share Vitamin D March 2012Документ7 страницSouthern Derbyshire Share Vitamin D March 2012dr rashid khanОценок пока нет
- Presentation DДокумент18 страницPresentation DGauravPathaniaОценок пока нет
- 11 2016 Prevention and Treatment of Vitamin D and Calcium Deficiency inДокумент7 страниц11 2016 Prevention and Treatment of Vitamin D and Calcium Deficiency insheyla alegreОценок пока нет
- Easy To ReadДокумент73 страницыEasy To Readdaljit chahalОценок пока нет
- Nutritional Considerations For Healthy Aging and Reduction in Age-Related Chronic DiseaseДокумент10 страницNutritional Considerations For Healthy Aging and Reduction in Age-Related Chronic DiseaseSilvana RamosОценок пока нет
- Society Achievers April 2023Документ108 страницSociety Achievers April 2023magnatepublishingpvtltdОценок пока нет
- The Skincarefalsepdf PDFДокумент8 страницThe Skincarefalsepdf PDFTeraОценок пока нет
- Everyday ScienceДокумент117 страницEveryday ScienceFawad Hayat MohmandОценок пока нет
- Skripsi Jonathan Darell Widjaja 1206230025Документ41 страницаSkripsi Jonathan Darell Widjaja 1206230025Jonathan Darell WijayaОценок пока нет
- Suplements in RehabДокумент20 страницSuplements in RehabpetrОценок пока нет
- 100 Passage Based Biology QuestionsДокумент17 страниц100 Passage Based Biology QuestionsMahmoud EbaidОценок пока нет
- Community Medicine Solved BCQs 8th Semester MBBS LUMHS-1Документ27 страницCommunity Medicine Solved BCQs 8th Semester MBBS LUMHS-1rameez ahmedОценок пока нет
- Vasvi and Vardah CC Report (1) .DocxkkkkkkkДокумент35 страницVasvi and Vardah CC Report (1) .Docxkkkkkkk9810102550aОценок пока нет