Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Executive Compensation at General Electric - Case StudyДокумент4 страницыExecutive Compensation at General Electric - Case StudyTupicica Gabriel100% (2)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Product Sheet - Parsys Cloud - Parsys TelemedicineДокумент10 страницProduct Sheet - Parsys Cloud - Parsys TelemedicineChristian Lezama Cuellar100% (1)
- Harmonized Household Profiling ToolДокумент2 страницыHarmonized Household Profiling ToolJessa Mae89% (9)
- German Specification BGR181 (English Version) - Acceptance Criteria For Floorings R Rating As Per DIN 51130Документ26 страницGerman Specification BGR181 (English Version) - Acceptance Criteria For Floorings R Rating As Per DIN 51130Ankur Singh ANULAB100% (2)
- Fundamentals of Financial ServicesДокумент16 страницFundamentals of Financial ServicesTupicica GabrielОценок пока нет
- Registration Quick Reference Card For Employees/AssociatesДокумент4 страницыRegistration Quick Reference Card For Employees/AssociatesTupicica GabrielОценок пока нет
- Referat 1Документ3 страницыReferat 1Tupicica GabrielОценок пока нет
- 31 639 Ap0 Composite Sink With Drainer: Descrierea ProdusuluiДокумент2 страницы31 639 Ap0 Composite Sink With Drainer: Descrierea ProdusuluiTupicica GabrielОценок пока нет
- EnergyLabel EFP60460OXДокумент1 страницаEnergyLabel EFP60460OXTupicica GabrielОценок пока нет
- EnergyLabel EZB5430ANXДокумент1 страницаEnergyLabel EZB5430ANXTupicica GabrielОценок пока нет
- 99 TVДокумент6 страниц99 TVTupicica GabrielОценок пока нет
- Set 878 Aqua: Product DescriptionДокумент2 страницыSet 878 Aqua: Product DescriptionTupicica GabrielОценок пока нет
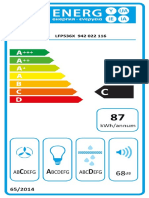
- EnergyLabel LFP536XДокумент1 страницаEnergyLabel LFP536XTupicica GabrielОценок пока нет
- Ce 420Документ24 страницыCe 420Tupicica GabrielОценок пока нет
- Chvartszaid David 201103 MSC ThesisДокумент153 страницыChvartszaid David 201103 MSC ThesisTupicica Gabriel100% (1)
- A Comm LogДокумент1 страницаA Comm LogTupicica GabrielОценок пока нет
- Laptopuri GabrielДокумент20 страницLaptopuri GabrielTupicica GabrielОценок пока нет
- A Review and Proposed A Criteria of Success - Albrektson Et AlДокумент39 страницA Review and Proposed A Criteria of Success - Albrektson Et AlTupicica GabrielОценок пока нет
- The Influence of Zirconia Coping Designs On The Fracture Load of All-Ceramic Molar CrownsДокумент17 страницThe Influence of Zirconia Coping Designs On The Fracture Load of All-Ceramic Molar CrownsTupicica GabrielОценок пока нет
- 99Документ21 страница99Tupicica GabrielОценок пока нет
- The Influence of Zirconia Coping Designs On The Fracture Load of All-Ceramic Molar CrownsДокумент12 страницThe Influence of Zirconia Coping Designs On The Fracture Load of All-Ceramic Molar CrownsTupicica GabrielОценок пока нет
- OA Standard 050505Документ75 страницOA Standard 050505fido_dagemОценок пока нет
- Reference Document GOIДокумент2 страницыReference Document GOIPranav BadrakiaОценок пока нет
- Practice Problems Mat Bal With RXNДокумент4 страницыPractice Problems Mat Bal With RXNRugi Vicente RubiОценок пока нет
- 2008 NOHC - JPHDSupplementДокумент62 страницы2008 NOHC - JPHDSupplementEliza DNОценок пока нет
- Equine Anesthesia Course NotesДокумент15 страницEquine Anesthesia Course NotesSam Bot100% (1)
- SSN Melaka SMK Seri Kota 2021 Annual Training Plan: Athletes Name Training ObjectivesДокумент2 страницыSSN Melaka SMK Seri Kota 2021 Annual Training Plan: Athletes Name Training Objectivessiapa kahОценок пока нет
- 4th Summative Science 6Документ2 страницы4th Summative Science 6brian blase dumosdosОценок пока нет
- The Benefits of RunningДокумент1 страницаThe Benefits of Runningefendi odidОценок пока нет
- Phenotype and GenotypeДокумент7 страницPhenotype and GenotypeIrish Claire Molina TragicoОценок пока нет
- The Chemical Composition and Organoleptic Attributes of Lesser-Known Vegetables As Consumed in Njikoka Local Government Area, Anambra State, NigeriaДокумент4 страницыThe Chemical Composition and Organoleptic Attributes of Lesser-Known Vegetables As Consumed in Njikoka Local Government Area, Anambra State, NigeriaEmri CynthiaОценок пока нет
- II092 - Horiz & Vert ULSs With Serial InputsДокумент4 страницыII092 - Horiz & Vert ULSs With Serial InputsJibjab7Оценок пока нет
- Moderated Caucus Speech Samples For MUNДокумент2 страницыModerated Caucus Speech Samples For MUNihabОценок пока нет
- Pengaruh Penambahan Lateks Pada Campuran Asphalt Concrete Binder Course (AC-BC)Документ10 страницPengaruh Penambahan Lateks Pada Campuran Asphalt Concrete Binder Course (AC-BC)Haris FirdausОценок пока нет
- Crime Free Lease AddendumДокумент1 страницаCrime Free Lease AddendumjmtmanagementОценок пока нет
- What Is Emergency ManagementДокумент8 страницWhat Is Emergency ManagementHilina hailuОценок пока нет
- 感應馬達安裝、保養使用說明書31057H402E (英)Документ17 страниц感應馬達安裝、保養使用說明書31057H402E (英)Rosyad Broe CaporegimeОценок пока нет
- Mapeh 9 Aho Q2W1Документ8 страницMapeh 9 Aho Q2W1Trisha Joy Paine TabucolОценок пока нет
- Workshop Manual Transporter 2016 19-29Документ157 страницWorkshop Manual Transporter 2016 19-29samueleОценок пока нет
- Cooling Tower (Genius)Документ7 страницCooling Tower (Genius)JeghiОценок пока нет
- Lead Avr PDFДокумент9 страницLead Avr PDFsiddharthОценок пока нет
- Liquid Enema ProcedureДокумент3 страницыLiquid Enema Procedureapi-209728657Оценок пока нет
- Mbs KatalogДокумент68 страницMbs KatalogDobroslav SoskicОценок пока нет
- 2017 LT4 Wiring DiagramДокумент10 страниц2017 LT4 Wiring DiagramThomasОценок пока нет
- SM FBD 70Документ72 страницыSM FBD 70LebahMadu100% (1)
- Fittings: Fitting Buying GuideДокумент2 страницыFittings: Fitting Buying GuideAaron FonsecaОценок пока нет
- Distribución Del Mercurio Total en Pescados y Mariscos Del Mar ArgentinoДокумент15 страницDistribución Del Mercurio Total en Pescados y Mariscos Del Mar ArgentinoaldiОценок пока нет
- Ineffective Breastfeeding - NCPДокумент10 страницIneffective Breastfeeding - NCPJullian PloyaОценок пока нет