Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Dieting Cheat Sheet Coach KyleДокумент2 страницыDieting Cheat Sheet Coach KyleMarcusОценок пока нет
- IMAT 2017 Humanitas - KEY A PAPERДокумент35 страницIMAT 2017 Humanitas - KEY A PAPERPascal KoureliasОценок пока нет
- Beachbody Diet Guide PDFДокумент8 страницBeachbody Diet Guide PDFIbad MohammedОценок пока нет
- ISSA Personal Trainer Certification Course Quizzes Ninth EditionДокумент35 страницISSA Personal Trainer Certification Course Quizzes Ninth Editionscorpion99938% (8)
- PE For SHS Grade 11 LM v3 PDFДокумент76 страницPE For SHS Grade 11 LM v3 PDFChristine Jane Ramos88% (8)
- Jchang 3-27casestudyinfertility TCMWT LNДокумент33 страницыJchang 3-27casestudyinfertility TCMWT LNdrprasantОценок пока нет
- Clinic Theater 2 - Class 5Документ2 страницыClinic Theater 2 - Class 5drprasant100% (1)
- Esu Tungintroim LN TCMWTДокумент8 страницEsu Tungintroim LN TCMWTdrprasant100% (1)
- GSG 8110 Blackberry ZenДокумент50 страницGSG 8110 Blackberry Zena99pОценок пока нет
- Clinic Theater 2 - Class 4Документ2 страницыClinic Theater 2 - Class 4drprasantОценок пока нет
- Clinic Theater 2 - Class 1Документ4 страницыClinic Theater 2 - Class 1drprasant100% (1)
- Dkaraba Neijing TCMWT HandoutДокумент16 страницDkaraba Neijing TCMWT HandoutdrprasantОценок пока нет
- Levatan Migraine TCMWT LNДокумент8 страницLevatan Migraine TCMWT LNdrprasantОценок пока нет
- Fen Touch Insert 27 Dec 2010Документ2 страницыFen Touch Insert 27 Dec 2010drprasantОценок пока нет
- Class 1Документ5 страницClass 1drprasantОценок пока нет
- Presenting: (Diclofenac Diethylamine B.P. 100 MG)Документ2 страницыPresenting: (Diclofenac Diethylamine B.P. 100 MG)drprasantОценок пока нет
- Clinic Theater 2 - Class 3Документ3 страницыClinic Theater 2 - Class 3drprasantОценок пока нет
- Dkaraba Introhowacu LN TCMWTДокумент20 страницDkaraba Introhowacu LN TCMWTdrprasantОценок пока нет
- Diagnostics I - PulsesДокумент15 страницDiagnostics I - Pulsesg23164100% (1)
- Study Notes - Exam 2Документ13 страницStudy Notes - Exam 2drprasantОценок пока нет
- Study Notes - Exam 1Документ8 страницStudy Notes - Exam 1drprasantОценок пока нет
- Advised Rest and If Required Low Intensity Light Activities During The Period of T/T of 10-12 DaysДокумент2 страницыAdvised Rest and If Required Low Intensity Light Activities During The Period of T/T of 10-12 Daysdrprasant100% (1)
- Given The Code in The Exhibit What Is The Result? A. B. C. D. Answer: B Explanation: ZДокумент1 страницаGiven The Code in The Exhibit What Is The Result? A. B. C. D. Answer: B Explanation: ZdrprasantОценок пока нет
- Presenting: (Ketoprofen I.P. 20 MG)Документ2 страницыPresenting: (Ketoprofen I.P. 20 MG)drprasantОценок пока нет
- Clinic Theater 2 - Class 2Документ4 страницыClinic Theater 2 - Class 2drprasantОценок пока нет
- Phase I: Power 90X - Classic Routine WorkoutДокумент42 страницыPhase I: Power 90X - Classic Routine WorkoutThomasToeshОценок пока нет
- American Accent Training ProgramДокумент74 страницыAmerican Accent Training ProgramAhmed Ra'efОценок пока нет
- Capri Institute of Manual Therapy: Address For Correspondence: - A-64, Hans Apartment, East Arjun Nagar, CBDДокумент1 страницаCapri Institute of Manual Therapy: Address For Correspondence: - A-64, Hans Apartment, East Arjun Nagar, CBDdrprasantОценок пока нет
- Muscle Energy TechniqueДокумент3 страницыMuscle Energy TechniquedrprasantОценок пока нет
- French Physical Therapy Technique Effective in Patients With Refractory Chronic Back PainДокумент1 страницаFrench Physical Therapy Technique Effective in Patients With Refractory Chronic Back PaindrprasantОценок пока нет
- Ma Ib 1013Документ72 страницыMa Ib 1013Shweta Jadhav-PatilОценок пока нет
- Applications Are Invited For The Following Class III Posts.: Mumbai Port TrustДокумент4 страницыApplications Are Invited For The Following Class III Posts.: Mumbai Port TrustPrashant SharmaОценок пока нет
- Tata Institute of Social Sciences Prospectus 2011-2013Документ74 страницыTata Institute of Social Sciences Prospectus 2011-2013navagatОценок пока нет
- Bill Barad BodybuilderДокумент9 страницBill Barad BodybuilderGolden Era BookwormОценок пока нет
- 7B Muscles, Movement and The Heart 7B CheckpointДокумент8 страниц7B Muscles, Movement and The Heart 7B CheckpointsalmaОценок пока нет
- MMMДокумент182 страницыMMMAlastair Harris100% (2)
- Raw Vegan PDFДокумент107 страницRaw Vegan PDFagrelot86% (7)
- FRF CrossCircuitTrainingДокумент27 страницFRF CrossCircuitTrainingJulio Olmedo100% (1)
- Chad Waterbury - Muscle RevolutionДокумент293 страницыChad Waterbury - Muscle RevolutionBigNat777486% (7)
- Physical Education 12 Dance: Name: Jenalyn Bugaay Grade 12 - Abm AДокумент8 страницPhysical Education 12 Dance: Name: Jenalyn Bugaay Grade 12 - Abm AJenalyn BugaayОценок пока нет
- IndividualityДокумент2 страницыIndividualityMiyangОценок пока нет
- Physiology of Muscle ContractionДокумент78 страницPhysiology of Muscle ContractionLenny MerdhaОценок пока нет
- The Muscle Pump Potential Mechanisms and ApplicationsДокумент6 страницThe Muscle Pump Potential Mechanisms and ApplicationsDan InsignaresОценок пока нет
- Gross Motor SkillsДокумент8 страницGross Motor SkillsLacra Apetrei100% (1)
- The Benefits of ExerciseДокумент21 страницаThe Benefits of ExerciseJay R BayaniОценок пока нет
- Sahya Part 4Документ116 страницSahya Part 4Homeopathy Torrents100% (1)
- Lec6 - Circulatory SystemДокумент4 страницыLec6 - Circulatory SystemEloisa Trina GenerosoОценок пока нет
- Massage Professional Ebook, 2nd EditionДокумент188 страницMassage Professional Ebook, 2nd EditionAnh Nguyễn33% (3)
- S6 Biology SB August 2018Документ421 страницаS6 Biology SB August 2018UMUFASHA Ange Justifiee100% (1)
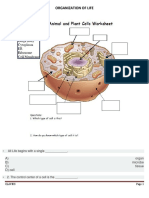
- Organization of LifeДокумент6 страницOrganization of LifeVina SihombingОценок пока нет
- Anatomy and Physiology Assignment 1Документ8 страницAnatomy and Physiology Assignment 1api-238869728Оценок пока нет
- Body Composition and Public Safety: The Industrial AthleteДокумент13 страницBody Composition and Public Safety: The Industrial AthleteAlireza GhanbariОценок пока нет
- Cinnamon Water: Preparation Category Synonyms Description of Final Product Use/s IngredientsДокумент6 страницCinnamon Water: Preparation Category Synonyms Description of Final Product Use/s IngredientsMaan EspirituОценок пока нет
- Akkaya 2012Документ13 страницAkkaya 2012Luis MiguelОценок пока нет
- Kinesiology Exam ReviewДокумент13 страницKinesiology Exam Reviewazn_taiwen8100% (1)
- The A to Z of Sprinting: A Guide to Multi-Year DevelopmentДокумент5 страницThe A to Z of Sprinting: A Guide to Multi-Year DevelopmentZachary LeeОценок пока нет
- Consenso de MunichДокумент10 страницConsenso de MunichBartholomew AllenОценок пока нет
- Core Stability and Bicycling: TrainingДокумент6 страницCore Stability and Bicycling: TrainingpehipsОценок пока нет
- HSB January 2019 Paper 2Документ24 страницыHSB January 2019 Paper 2Chitra Snow0% (1)