Вам также может понравиться
- Neonatal SeizuresДокумент4 страницыNeonatal SeizuresSerag EdeenОценок пока нет
- Basics Principle and Guidelines To Neonatal VentilationДокумент5 страницBasics Principle and Guidelines To Neonatal VentilationMaria Babette Almazan TalaveraОценок пока нет
- Nursing the NeonateОт EverandNursing the NeonateMaggie MeeksОценок пока нет
- 21321Документ56 страниц21321Daniel TabalanzaОценок пока нет
- Management and Care of Sick NeonateДокумент30 страницManagement and Care of Sick NeonateYashvi SinghОценок пока нет
- Premature Baby AssessmentДокумент20 страницPremature Baby AssessmentSREEDEVI T SURESHОценок пока нет
- 05 Polycythemia in The NewbornДокумент11 страниц05 Polycythemia in The NewbornMorales Eli PediatraОценок пока нет
- Neonatal Hypoglycemia: 1.transient (Most Common) 2.persistenet (Less Common)Документ8 страницNeonatal Hypoglycemia: 1.transient (Most Common) 2.persistenet (Less Common)mohammadОценок пока нет
- 4nursing Care of Newborn and FamilyДокумент15 страниц4nursing Care of Newborn and FamilyMary RoseОценок пока нет
- Skills For Care Presentation Web Version Standard 3Документ16 страницSkills For Care Presentation Web Version Standard 3pitr134Оценок пока нет
- PrematurityДокумент37 страницPrematuritySolomon AmosОценок пока нет
- What Is The Glasgow Coma Scale?: BrainlineДокумент4 страницыWhat Is The Glasgow Coma Scale?: BrainlineHershey ArenasОценок пока нет
- NicuДокумент35 страницNicuJaya Prabha100% (2)
- Clinical Approach To Respiratory Distress in NewbornДокумент29 страницClinical Approach To Respiratory Distress in Newbornabhivnair100% (1)
- Neonatal Transition: Training of The Trainers Neonatal ResuscitationДокумент36 страницNeonatal Transition: Training of The Trainers Neonatal ResuscitationmitaОценок пока нет
- Neonatal SubgalealДокумент6 страницNeonatal SubgalealIrenLayОценок пока нет
- 1 - Fetal Physiology and The Transition To Extrauterine LifeДокумент13 страниц1 - Fetal Physiology and The Transition To Extrauterine LifeRonaldo Pineda WieselbergОценок пока нет
- 2020 Neonata Lcare PDFДокумент20 страниц2020 Neonata Lcare PDFserigne badianeОценок пока нет
- Neonatal Ventilation PDFДокумент29 страницNeonatal Ventilation PDFIsabella HosanaОценок пока нет
- Neonatal ThermoregulationДокумент4 страницыNeonatal Thermoregulationalicia618Оценок пока нет
- Febrile SeizuresДокумент18 страницFebrile Seizureskara_korum100% (1)
- Newborn Respiratory Disorders PDFДокумент10 страницNewborn Respiratory Disorders PDFMax RodriguezОценок пока нет
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Meconium Aspiration SyndromeДокумент7 страницMeconium Aspiration SyndromeAi Niech Inoel100% (1)
- Care of Low Birth Weight (LBW) BabiesДокумент44 страницыCare of Low Birth Weight (LBW) BabiesSubhajit Ghosh100% (1)
- Essential Newborn CareДокумент14 страницEssential Newborn CareJam Corros100% (1)
- Pediatric Newborn Medicine Clinical Practice GuidelinesДокумент15 страницPediatric Newborn Medicine Clinical Practice GuidelinesJosselle Sempio CalientaОценок пока нет
- Management of Neonatal HypoglycemiaДокумент14 страницManagement of Neonatal Hypoglycemiaece142Оценок пока нет
- Birth AsphyxiaДокумент20 страницBirth Asphyxiainne_fОценок пока нет
- Lecture 1 Mechanical Ventilation An IntroductionДокумент20 страницLecture 1 Mechanical Ventilation An IntroductionEng Kian NgОценок пока нет
- Bronchiolitis PDFДокумент7 страницBronchiolitis PDFYoerizta RatuОценок пока нет
- Newborn Assessment Period: ST THДокумент3 страницыNewborn Assessment Period: ST THYoussef AliОценок пока нет
- Pediatric Emergencies PDFДокумент20 страницPediatric Emergencies PDFOxana Turcu100% (1)
- Golden Hours Management of High Risk Newborns - 2019Документ10 страницGolden Hours Management of High Risk Newborns - 2019Suryadi LimardiОценок пока нет
- Hypoxic Ischemic Encephalopathy Updates in ManagementДокумент67 страницHypoxic Ischemic Encephalopathy Updates in Managementlordoftheweb100% (7)
- Neonatal SepsisДокумент17 страницNeonatal SepsisDhilla Feroh Kesuma TОценок пока нет
- Resuscitation of New Born: SBA - Presentation 5 (B)Документ27 страницResuscitation of New Born: SBA - Presentation 5 (B)Dr-Nikhil Goswami100% (1)
- Chronic Cough In Children, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandChronic Cough In Children, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- MeningitisДокумент12 страницMeningitisFaith Vaughn100% (2)
- 1.conginital Cardiac DefectsДокумент39 страниц1.conginital Cardiac DefectsJõsëph Jåy MîthОценок пока нет
- Fluid Management in Neonates and InfantsДокумент51 страницаFluid Management in Neonates and InfantsSulabh Shrestha100% (1)
- Examination of Newborn Physical Examination Include The FollowingДокумент34 страницыExamination of Newborn Physical Examination Include The FollowingZimm Rrrr100% (2)
- Congenital AnomaliesДокумент22 страницыCongenital Anomaliesjessy100% (1)
- Neonatal HypocalcemiaДокумент8 страницNeonatal HypocalcemiaCristina Fernández ValenciaОценок пока нет
- Neonatal SeizuresДокумент26 страницNeonatal SeizuresStrept PneumoniaОценок пока нет
- Neonatal GoalsДокумент5 страницNeonatal GoalsJehanie LukmanОценок пока нет
- EngДокумент54 страницыEngAiralyn Chavez Alaro100% (1)
- Neonatal Seizures: Current Management and Future ChallengesОт EverandNeonatal Seizures: Current Management and Future ChallengesLakshmi NagarajanРейтинг: 4 из 5 звезд4/5 (2)
- Neonatal Hypocalcemia: Presented By: Ms. Manisha Thakur Nursing Tutor Child Health NursingДокумент11 страницNeonatal Hypocalcemia: Presented By: Ms. Manisha Thakur Nursing Tutor Child Health Nursingmanisha thakurОценок пока нет
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuДокумент31 страницаNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanОценок пока нет
- Delayed Vs Immediate Umbilical Cord ClampingДокумент37 страницDelayed Vs Immediate Umbilical Cord ClampingAndi DeviriyantiОценок пока нет
- Hypoxic Ischemic EncephalopathyДокумент7 страницHypoxic Ischemic EncephalopathyJennesse May Guiao IbayОценок пока нет
- Respiratory Distress Management in NewbornДокумент5 страницRespiratory Distress Management in Newbornagirl_9807100% (1)
- Neonatal Resuscitation. Advances in Training and PracticeДокумент10 страницNeonatal Resuscitation. Advances in Training and PracticeFer45Оценок пока нет
- ALLERGIC RHINITIS IN CHILDREN RinaДокумент39 страницALLERGIC RHINITIS IN CHILDREN Rinarinajacky100% (2)
- Hemorrhagic Disease of Newborn PDFДокумент2 страницыHemorrhagic Disease of Newborn PDFIndah Paradifa SariОценок пока нет
- The Nurse Practitioner in UrologyОт EverandThe Nurse Practitioner in UrologyMichelle LajinessОценок пока нет
- Neonatal Golden HourДокумент28 страницNeonatal Golden HourGendis Ayu ArdiasОценок пока нет
- Management and Investigation of Neonatal Encephalopathy: 2017 UpdateДокумент13 страницManagement and Investigation of Neonatal Encephalopathy: 2017 Updatenuge putriОценок пока нет
- Mechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeДокумент12 страницMechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeGayathri RОценок пока нет
- A Sample Script For Public SpeakingДокумент2 страницыA Sample Script For Public Speakingalmasodi100% (2)
- Cs Fujitsu SAP Reference Book IPDFДокумент63 страницыCs Fujitsu SAP Reference Book IPDFVijay MindfireОценок пока нет
- Merchant Shipping MINIMUM SAFE MANNING Regulations 2016Документ14 страницMerchant Shipping MINIMUM SAFE MANNING Regulations 2016Arthur SchoutОценок пока нет
- Conjunctions in SentencesДокумент8 страницConjunctions in SentencesPunitha PoppyОценок пока нет
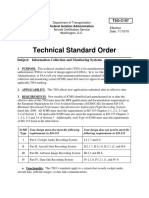
- Tso C197Документ6 страницTso C197rdpereirОценок пока нет
- Rule 7bДокумент38 страницRule 7bKurt ReoterasОценок пока нет
- 506 Koch-Glitsch PDFДокумент11 страниц506 Koch-Glitsch PDFNoman Abu-FarhaОценок пока нет
- Growing Onion Management and Water NeedsДокумент25 страницGrowing Onion Management and Water NeedsKATE NAVAJAОценок пока нет
- Modular ResumeДокумент1 страницаModular ResumeedisontОценок пока нет
- PrimerCube Manufacturing GuideДокумент57 страницPrimerCube Manufacturing GuideTinaMaleenaОценок пока нет
- Plant Vs Filter by Diana WalstadДокумент6 страницPlant Vs Filter by Diana WalstadaachuОценок пока нет
- Wordbank 15 Youtube Writeabout1Документ2 страницыWordbank 15 Youtube Writeabout1Olga VaizburgОценок пока нет
- PBPO008E FrontmatterДокумент13 страницPBPO008E FrontmatterParameswararao Billa67% (3)
- Accounting System (Compatibility Mode) PDFДокумент10 страницAccounting System (Compatibility Mode) PDFAftab AlamОценок пока нет
- Abacus 1 PDFДокумент13 страницAbacus 1 PDFAli ChababОценок пока нет
- MSDS Charcoal Powder PDFДокумент3 страницыMSDS Charcoal Powder PDFSelina VdexОценок пока нет
- Crown BeverageДокумент13 страницCrown BeverageMoniruzzaman JurorОценок пока нет
- Old Highland Park Baptist Church E01Документ74 страницыOld Highland Park Baptist Church E01Lawrence Garner100% (2)
- Polyembryony &its ImportanceДокумент17 страницPolyembryony &its ImportanceSURIYA PRAKASH GОценок пока нет
- Internal Gear Pump: Replaces: 03.08 Material No. R901216585 Type PGH.-3XДокумент36 страницInternal Gear Pump: Replaces: 03.08 Material No. R901216585 Type PGH.-3XbiabamanbemanОценок пока нет
- Unit 2 Operations of PolynomialsДокумент28 страницUnit 2 Operations of Polynomialsapi-287816312Оценок пока нет
- DescriptiveДокумент1 страницаDescriptiveRizqa Anisa FadhilahОценок пока нет
- TV Antenna Tower CollapseДокумент4 страницыTV Antenna Tower CollapseImdaad ChuubbОценок пока нет
- Adhesive Film & TapeДокумент6 страницAdhesive Film & TapeJothi Vel MuruganОценок пока нет
- A Vision System For Surface Roughness Characterization Using The Gray Level Co-Occurrence MatrixДокумент12 страницA Vision System For Surface Roughness Characterization Using The Gray Level Co-Occurrence MatrixPraveen KumarОценок пока нет
- HUAWEI PowerCube 500Документ41 страницаHUAWEI PowerCube 500soumen95Оценок пока нет
- FMO ESG Toolkit (AutoRecovered)Документ149 страницFMO ESG Toolkit (AutoRecovered)me.abhishekpОценок пока нет
- Amsterdam Pipe Museum - Snuff WorldwideДокумент1 страницаAmsterdam Pipe Museum - Snuff Worldwideevon1Оценок пока нет
- M.T Nautica Batu Pahat: Clean Product Tanker 4,497 BHPДокумент1 страницаM.T Nautica Batu Pahat: Clean Product Tanker 4,497 BHPSuper 247Оценок пока нет
- Letter of Acceptfor TДокумент3 страницыLetter of Acceptfor TCCSОценок пока нет