Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Risk Assessment For Installation of Toilet Exhaust FanДокумент11 страницRisk Assessment For Installation of Toilet Exhaust FanAnandu Ashokan67% (3)
- CPC First TestДокумент102 страницыCPC First TestChinnammal M100% (2)
- Anatomical Terms: I. Anatomic VariationДокумент8 страницAnatomical Terms: I. Anatomic VariationNellen BastismoОценок пока нет
- People v. Dalag y Custodio 402 SCRA 254 PDFДокумент27 страницPeople v. Dalag y Custodio 402 SCRA 254 PDFfelix camerinoОценок пока нет
- Dca CPT CodesДокумент1 страницаDca CPT CodesaninnaОценок пока нет
- Overgranulation: A. Muhammad Reva A.MДокумент21 страницаOvergranulation: A. Muhammad Reva A.Mgalih widodoОценок пока нет
- Flyer Asmpid 2021Документ2 страницыFlyer Asmpid 2021Agus WijataОценок пока нет
- Nna en November09Документ3 страницыNna en November09Agus WijataОценок пока нет
- Kids Games Powerpoint TemplateДокумент26 страницKids Games Powerpoint TemplateAgus WijataОценок пока нет
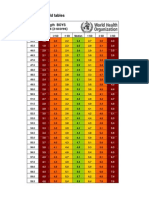
- WHO New Zscore WLZ Boys 0-2yrsДокумент5 страницWHO New Zscore WLZ Boys 0-2yrsAgus WijataОценок пока нет
- Status of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaДокумент4 страницыStatus of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaAgus WijataОценок пока нет
- Espr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedДокумент1 страницаEspr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedAgus WijataОценок пока нет
- Early Biochemical Indicators of Hypoxic-Ischemic Encephalopathy After Birth AsphyxiaДокумент5 страницEarly Biochemical Indicators of Hypoxic-Ischemic Encephalopathy After Birth AsphyxiaAgus WijataОценок пока нет
- Neuron-Specific Enolase As A Marker of The Severity and Outcome of Hypoxic Ischemic EncephalopathyДокумент5 страницNeuron-Specific Enolase As A Marker of The Severity and Outcome of Hypoxic Ischemic EncephalopathyAgus WijataОценок пока нет
- Edwin Kim, MD A. Wesley Burks, MD Michael Pistiner, MD, MMSCДокумент1 страницаEdwin Kim, MD A. Wesley Burks, MD Michael Pistiner, MD, MMSCAgus WijataОценок пока нет
- Biochemical Marker As Predictor of Outcome in Perinatal AsphyxiaДокумент4 страницыBiochemical Marker As Predictor of Outcome in Perinatal AsphyxiaAgus WijataОценок пока нет
- Bloody DДокумент31 страницаBloody DAgus WijataОценок пока нет
- KBM0701 Stern 21Документ6 страницKBM0701 Stern 21Agus WijataОценок пока нет
- MML Test Setup PDFДокумент1 страницаMML Test Setup PDFAgus WijataОценок пока нет
- Scaphoid Fracture - Overview and Conservative Treatment PDFДокумент7 страницScaphoid Fracture - Overview and Conservative Treatment PDFCamilo VidalОценок пока нет
- Vizcarrondo Rios Vs NYC Dept of EducationДокумент26 страницVizcarrondo Rios Vs NYC Dept of EducationErin LaviolaОценок пока нет
- Guard DutyДокумент23 страницыGuard DutynotbowenОценок пока нет
- Julius and The WatchmakerДокумент388 страницJulius and The WatchmakerLuisa Agnese Dalla FontanaОценок пока нет
- Kettle Bell Workout RoutineДокумент3 страницыKettle Bell Workout RoutinemotmagicОценок пока нет
- 1920 1924Документ16 страниц1920 1924api-246211793Оценок пока нет
- Fireworks Bangs Lake Park ExplosionДокумент9 страницFireworks Bangs Lake Park Explosionfickes1307Оценок пока нет
- Jurnal Fr. PatellaДокумент13 страницJurnal Fr. PatellaSlluada UntkmuwОценок пока нет
- Job Hazard Analysis - TubingsДокумент9 страницJob Hazard Analysis - TubingsJayson Escamillan100% (1)
- Brachial Plexus InjuryДокумент10 страницBrachial Plexus InjurySanditya FadliОценок пока нет
- Anatomy of The LegДокумент39 страницAnatomy of The LegUzma KhanОценок пока нет
- GWC Small BallДокумент16 страницGWC Small BallApresia KiranaОценок пока нет
- Case Study ON: Acute Spinal Cord InjuryДокумент49 страницCase Study ON: Acute Spinal Cord InjuryJM RomiasОценок пока нет
- 1 Introduction To TCCC USA 20015Документ47 страниц1 Introduction To TCCC USA 20015Jorge Almeida CostaОценок пока нет
- 2015-03-14 - Operation Instructions High-Z S-1400T Series - EN PDFДокумент81 страница2015-03-14 - Operation Instructions High-Z S-1400T Series - EN PDFAnonymous NFKwjkHvkОценок пока нет
- Negligence in Construction and MedicalДокумент8 страницNegligence in Construction and Medicalmariatul3056Оценок пока нет
- Slinging LoadsДокумент2 страницыSlinging LoadsDang Minh HuongОценок пока нет
- Pe & Health 6-25-14 PDFДокумент432 страницыPe & Health 6-25-14 PDFRomeo D Belnas0% (1)
- HemophiliaДокумент31 страницаHemophiliaspica25Оценок пока нет
- Flying in 4Документ108 страницFlying in 4Julio Olvera100% (3)
- Mourngul: Description AbilitiesДокумент1 страницаMourngul: Description AbilitiesFininОценок пока нет
- Naval SERE Survival Handbook (1970s)Документ79 страницNaval SERE Survival Handbook (1970s)RobertMiletich100% (6)
- Astray (Gated Sequel) by Amy Christine ParkerДокумент27 страницAstray (Gated Sequel) by Amy Christine ParkerRandom House TeensОценок пока нет
- Definitions and Data Availability: IrtadДокумент37 страницDefinitions and Data Availability: IrtadedduardocОценок пока нет