Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Dvet RCTДокумент7 страницDvet RCTJill PОценок пока нет
- Guidelines For Prophylaxis of HIV Exposed InfantsДокумент35 страницGuidelines For Prophylaxis of HIV Exposed InfantsJill PОценок пока нет
- Revised PubMat Guide To Breastfeeding - EnglishДокумент1 страницаRevised PubMat Guide To Breastfeeding - EnglishJill PОценок пока нет
- Antibiotics in Pediatrics (Vancomycin, Quinolones, Aminoglycosides, Tetracyclines, Chloramphenicol, Clindamycin, Macrolides)Документ90 страницAntibiotics in Pediatrics (Vancomycin, Quinolones, Aminoglycosides, Tetracyclines, Chloramphenicol, Clindamycin, Macrolides)Jill PОценок пока нет
- Allergo-Immunology Hour: Food AllergyДокумент32 страницыAllergo-Immunology Hour: Food AllergyJill PОценок пока нет
- What Is It For?: TCA Glycolysis Gluconeogenesis Glycogenesis Glycogenolysis PPPДокумент3 страницыWhat Is It For?: TCA Glycolysis Gluconeogenesis Glycogenesis Glycogenolysis PPPJill PОценок пока нет
- PPHCH 2012Документ41 страницаPPHCH 2012Jill P100% (1)
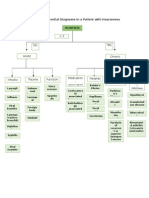
- General Differentials For Hoarseness (Concept Map)Документ1 страницаGeneral Differentials For Hoarseness (Concept Map)Jill PОценок пока нет
- IMCI Chart Booklet PDFДокумент80 страницIMCI Chart Booklet PDFmikay100% (1)
- Republic Act MnemonicsДокумент3 страницыRepublic Act MnemonicsJill P100% (1)
- Diabetes Mellitus During PregnancyДокумент75 страницDiabetes Mellitus During PregnancyJill PОценок пока нет
- Microscopic Descriptive TechniquesДокумент13 страницMicroscopic Descriptive TechniquesJill PОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- April 2009Документ19 страницApril 2009PROGNAS HIV RSBWОценок пока нет
- CVS Examination EditedДокумент134 страницыCVS Examination EditedThilak JayalathОценок пока нет
- Valvular DiseasesДокумент8 страницValvular DiseasesBeryl Ben MergalОценок пока нет
- AHA Examination Auscultation Part IVДокумент42 страницыAHA Examination Auscultation Part IVHananya ManroeОценок пока нет
- Cardiac SystemДокумент7 страницCardiac Systemsccctutor100% (3)
- Aortic Stenosis: Sherif EL Hawary, MDДокумент6 страницAortic Stenosis: Sherif EL Hawary, MDSyximsh FPОценок пока нет
- Head To Toe Physical Assessment ChecklistДокумент16 страницHead To Toe Physical Assessment ChecklistMichael Allen Fadriquel100% (10)
- Chapter 09Документ3 страницыChapter 09Teehee Jones100% (2)
- Biopac Lesson 17 ProcedureДокумент16 страницBiopac Lesson 17 ProcedureEdwin PurcellОценок пока нет
- Cardiovascular Examination A. 1. Wash Hands Before Touching Patient, B. 2. Explain What You Like To Do & ObtainДокумент2 страницыCardiovascular Examination A. 1. Wash Hands Before Touching Patient, B. 2. Explain What You Like To Do & ObtainDeepbluexОценок пока нет
- Cu 10 Cardiovascular SystemДокумент88 страницCu 10 Cardiovascular SystemRose MendozaОценок пока нет
- CardiomyopathyДокумент18 страницCardiomyopathyDimpal Choudhary100% (1)
- Short Cases in MedicineДокумент30 страницShort Cases in MedicineselamuОценок пока нет
- Cardiopulmonary Assessment 2020721956580Документ36 страницCardiopulmonary Assessment 2020721956580Kavya MittalОценок пока нет
- Cardio Intensive ReviewДокумент40 страницCardio Intensive ReviewAchilles YbarraОценок пока нет
- Head To Toe Assessment in 5 Minutes or MoreДокумент12 страницHead To Toe Assessment in 5 Minutes or MoreTSPANОценок пока нет
- Assessing Heart and Central VesselsДокумент34 страницыAssessing Heart and Central VesselsGemmalene Pacleb100% (1)
- Head To Toe Assessment Normal FindingsДокумент13 страницHead To Toe Assessment Normal FindingsDanica May Corpuz Comia-Enriquez100% (3)
- 3 Patient AssessmentДокумент499 страниц3 Patient AssessmentRaul GascueñaОценок пока нет
- Decreased Cardiac OutputДокумент4 страницыDecreased Cardiac OutputChristine MatasОценок пока нет
- Apical Pulse AssessmentДокумент9 страницApical Pulse AssessmentmscastrogelacastroОценок пока нет
- Notes On CVS and Respiratory ExaminationДокумент2 страницыNotes On CVS and Respiratory Examinationwel2332Оценок пока нет
- As CM Pre Clerkship HandbookДокумент164 страницыAs CM Pre Clerkship HandbookClarice Mae DacasinОценок пока нет
- NCLEX Practice Exam 21 (60 Questions)Документ36 страницNCLEX Practice Exam 21 (60 Questions)Melodia Turqueza GandezaОценок пока нет
- CH 11 Lecture Presentation Cardiovascular-System PDFДокумент132 страницыCH 11 Lecture Presentation Cardiovascular-System PDFNicole MagbanuaОценок пока нет
- All Uworld Notes 2019 Nclex Nursing ResourcesДокумент152 страницыAll Uworld Notes 2019 Nclex Nursing Resourcesnene lewis100% (1)
- Congenital Heart DiseasesДокумент52 страницыCongenital Heart DiseasesCristina Maria100% (1)
- WARDWORK TemplateДокумент9 страницWARDWORK TemplateColeen NeyraОценок пока нет
- Ecg Short Rapid ReviewДокумент54 страницыEcg Short Rapid ReviewSilviaSumintoОценок пока нет
- Health Assessment TransДокумент27 страницHealth Assessment TransPia Gabrielle CabatanaОценок пока нет