Вам также может понравиться
- Horowitz, Israel Albert - Reinfeld, Fred - How To Think Ahead in Chess - The Methods and Techniques of Planning Your Entire Game (1979, Simon and Schuster) PDFДокумент278 страницHorowitz, Israel Albert - Reinfeld, Fred - How To Think Ahead in Chess - The Methods and Techniques of Planning Your Entire Game (1979, Simon and Schuster) PDFRoberto HernandezОценок пока нет
- SSRN Id3407263 PDFДокумент40 страницSSRN Id3407263 PDFRoberto HernandezОценок пока нет
- Barth 2004Документ38 страницBarth 2004Roberto HernandezОценок пока нет
- Visual Birth Plan All IconsДокумент9 страницVisual Birth Plan All IconsRoberto HernandezОценок пока нет
- Sports Medicine Volume 40 Issue 3 2010 (Doi 10.2165/11319770-000000000-00000) Issurin, Vladimir B. - New Horizons For The Methodology and Physiology of Training PeriodizationДокумент18 страницSports Medicine Volume 40 Issue 3 2010 (Doi 10.2165/11319770-000000000-00000) Issurin, Vladimir B. - New Horizons For The Methodology and Physiology of Training PeriodizationRoberto HernandezОценок пока нет
- Optimal Portfolio Selection Without Short Sales Under The Full-Information Covariance Structure: A Pedagogic ConsiderationДокумент8 страницOptimal Portfolio Selection Without Short Sales Under The Full-Information Covariance Structure: A Pedagogic ConsiderationRoberto HernandezОценок пока нет
- Exposure CalculatorДокумент2 страницыExposure CalculatormcsuzanoОценок пока нет
- Remortgage Guide 2014Документ65 страницRemortgage Guide 2014Roberto HernandezОценок пока нет
- Consistent Dividend Growth Investment StrategiesДокумент25 страницConsistent Dividend Growth Investment StrategiesRoberto HernandezОценок пока нет
- Increasing Retention PashlerДокумент4 страницыIncreasing Retention PashlerRoberto HernandezОценок пока нет
- Worlds Greatest StretchДокумент1 страницаWorlds Greatest StretchRoberto HernandezОценок пока нет
- WP 4-2012 Amir KamaДокумент45 страницWP 4-2012 Amir KamaRoberto HernandezОценок пока нет
- Is The PEG Ratio A Valid ConceptДокумент5 страницIs The PEG Ratio A Valid ConceptRoberto HernandezОценок пока нет
- WP 4-2012 Amir KamaДокумент45 страницWP 4-2012 Amir KamaRoberto HernandezОценок пока нет
- Rucak Za 30 MinutaДокумент53 страницыRucak Za 30 MinutaRebecca ReevesОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
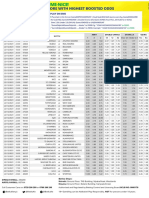
- Date Time Game Id Match 1 X 2 1X 12 X2 Over 2.5 Under 2.5 Yes NoДокумент2 страницыDate Time Game Id Match 1 X 2 1X 12 X2 Over 2.5 Under 2.5 Yes Nojust ANDROIDОценок пока нет
- Trekking Cuzco1Документ3 страницыTrekking Cuzco1Josue John Jaime CardenasОценок пока нет
- Sailing Hydrofoil: Typical Configurations Foiling ClassesДокумент5 страницSailing Hydrofoil: Typical Configurations Foiling ClassesbogdanОценок пока нет
- Toledo Mud Hens 2024 ScheduleДокумент1 страницаToledo Mud Hens 2024 ScheduleJake PietraszОценок пока нет
- Toyota 4runner Specifications Part 8 ManualДокумент8 страницToyota 4runner Specifications Part 8 ManualMiguel RamosОценок пока нет
- Philippine International Hot Air Balloon FiestaДокумент4 страницыPhilippine International Hot Air Balloon FiestaMark Edrian YumolОценок пока нет
- Lifting 101Документ3 страницыLifting 101api-302300769Оценок пока нет
- 50H - 50MДокумент437 страниц50H - 50MFran Chaf100% (1)
- Oxford Placement Test RespuestasДокумент4 страницыOxford Placement Test Respuestasclara100% (1)
- Toyota - PQMДокумент8 страницToyota - PQMAziz FroshОценок пока нет
- Chapter 21 Muscle Blood FlowДокумент17 страницChapter 21 Muscle Blood Flowelmedina omeragicОценок пока нет
- App c4 Design of SailplanesДокумент32 страницыApp c4 Design of SailplanesfakeОценок пока нет
- Royal EnfieldДокумент18 страницRoyal Enfieldram prasad das100% (1)
- Tactical MonsterДокумент15 страницTactical MonsterJovОценок пока нет
- 6.4 Rotational Kinetic Energy 1Документ5 страниц6.4 Rotational Kinetic Energy 1Keira BОценок пока нет
- (3.5 (ToB) PEACH) Solaris Arcanum - The Arcane Discipline Unearthed - Golden-Esque (GitP)Документ13 страниц(3.5 (ToB) PEACH) Solaris Arcanum - The Arcane Discipline Unearthed - Golden-Esque (GitP)RaphiezarОценок пока нет
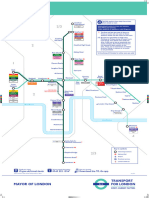
- DLR Route MapДокумент1 страницаDLR Route MapChristopher HollowayОценок пока нет
- Timing Belt: Service and Repair Timing Belt, DismantlingДокумент5 страницTiming Belt: Service and Repair Timing Belt, DismantlingGustavo Guzuck Gutierrez Gonzalez100% (1)
- Question Tags - Essay TaskДокумент1 страницаQuestion Tags - Essay TaskHidayatul HikmahОценок пока нет
- Sintesis 3ro Basico (Reparado)Документ11 страницSintesis 3ro Basico (Reparado)Bernardita Isabel Sánchez GodoyОценок пока нет
- Swiss Knitter & Passap Goldy ManualДокумент51 страницаSwiss Knitter & Passap Goldy ManualWilliam Phillip80% (5)
- 57 Pages - Thesis About Prediction of Cricket Match OutcomeДокумент57 страниц57 Pages - Thesis About Prediction of Cricket Match OutcomeJehanОценок пока нет
- Alternity and Star Frontiers Alien Species Conversions To SWN 01-06-2017Документ13 страницAlternity and Star Frontiers Alien Species Conversions To SWN 01-06-2017Andre Luiz JuniorОценок пока нет
- Burns - Airway Clearance, Risk For IneffectiveДокумент2 страницыBurns - Airway Clearance, Risk For Ineffectivemakyofrancis20Оценок пока нет
- Weekly Physical Activity Log SheetДокумент2 страницыWeekly Physical Activity Log SheetFast BlastОценок пока нет
- 1903 9485 95 - P-37 IvrДокумент48 страниц1903 9485 95 - P-37 IvrrsengineersОценок пока нет
- Operational InformationДокумент58 страницOperational InformationindonesiakujayaОценок пока нет
- Pe 111 CompleteДокумент69 страницPe 111 CompleteDanilo Jr Oribello Navaja100% (1)
- Reman-C10508567 Caterpillar RemanДокумент32 страницыReman-C10508567 Caterpillar RemanElmer Lagua Malpaso67% (3)
- Avenger 1 Play ImporДокумент12 страницAvenger 1 Play ImporJosé ChamayОценок пока нет