Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Paediatric Guidelines NewДокумент16 страницPaediatric Guidelines NewVitya ResanindyaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Eb SteinДокумент112 страницEb SteinAsena TuiketeiОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- TorchДокумент1 страницаTorchAsena TuiketeiОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Child TB Training Toolkit WebДокумент47 страницChild TB Training Toolkit WebAsena TuiketeiОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Pediatrics in Review 2010 Cruz 13 26Документ16 страницPediatrics in Review 2010 Cruz 13 26Asena TuiketeiОценок пока нет
- PIIS1071909114000072Документ7 страницPIIS1071909114000072Asena TuiketeiОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Pediatric TuberculosisДокумент36 страницPediatric TuberculosisAsena TuiketeiОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Pediatrics 2013 Jegatheesan E1803 10Документ10 страницPediatrics 2013 Jegatheesan E1803 10Asena TuiketeiОценок пока нет
- Eye Movements Clinical CorrelationДокумент8 страницEye Movements Clinical CorrelationAsena TuiketeiОценок пока нет
- Learn PediatricsДокумент5 страницLearn PediatricsAsena TuiketeiОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Neoreviews 2001 Enns E183 91Документ11 страницNeoreviews 2001 Enns E183 91Asena TuiketeiОценок пока нет
- 201 - Docctor I See DoubleДокумент8 страниц201 - Docctor I See DoubleAsena TuiketeiОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Arch Dis Child Fetal Neonatal Ed-2001-Chakrapani-F205-10Документ7 страницArch Dis Child Fetal Neonatal Ed-2001-Chakrapani-F205-10Asena TuiketeiОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Diagnosing Inborn Errors of Metabolism in The NewbornДокумент11 страницDiagnosing Inborn Errors of Metabolism in The NewbornAsena TuiketeiОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Arch Dis Child Fetal Neonatal Ed-2001-Chakrapani-F205-10Документ7 страницArch Dis Child Fetal Neonatal Ed-2001-Chakrapani-F205-10Asena TuiketeiОценок пока нет
- Turner Syndrome: A Guide For FamiliesДокумент32 страницыTurner Syndrome: A Guide For FamiliesAsena TuiketeiОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Resident Guide To Pediatric Rheumatology 2011Документ61 страницаResident Guide To Pediatric Rheumatology 2011Giorgi BradОценок пока нет
- Neonatal+sepsis June2014Документ14 страницNeonatal+sepsis June2014Asena TuiketeiОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Burns Guidelines 2010Документ45 страницBurns Guidelines 2010Asena TuiketeiОценок пока нет
- Burns Guidelines Quick Reference ChartДокумент1 страницаBurns Guidelines Quick Reference ChartAsena TuiketeiОценок пока нет
- Pediatric Burns Mortality Risk Factors in A Developing Country's Tertiary Burns Intensive Care Unit PDFДокумент8 страницPediatric Burns Mortality Risk Factors in A Developing Country's Tertiary Burns Intensive Care Unit PDFRisandy DitiaОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- A Comparative Study of The Effect of Different Topical Agents On Burn Wound InfectionsДокумент8 страницA Comparative Study of The Effect of Different Topical Agents On Burn Wound InfectionsAsena TuiketeiОценок пока нет
- 2.ed - Eng6 - q1 - Mod3 - Make Connections Between Information Viewed and Personal ExpiriencesДокумент32 страницы2.ed - Eng6 - q1 - Mod3 - Make Connections Between Information Viewed and Personal ExpiriencesToni Marie Atienza Besa100% (3)
- Unit 1 Bearer PlantsДокумент2 страницыUnit 1 Bearer PlantsEmzОценок пока нет
- Learning Competency PDFДокумент1 страницаLearning Competency PDFLEOMAR PEUGALОценок пока нет
- Initial Police Report: Calamba City Police Station Brgy Real, Calamba City, Laguna E-Mail: 545-1694/545-6789 Loc 8071Документ1 страницаInitial Police Report: Calamba City Police Station Brgy Real, Calamba City, Laguna E-Mail: 545-1694/545-6789 Loc 8071Jurish BunggoОценок пока нет
- Densha: Memories of A Train Ride Through Kyushu: By: Scott NesbittДокумент7 страницDensha: Memories of A Train Ride Through Kyushu: By: Scott Nesbittapi-16144421Оценок пока нет
- Ships Near A Rocky Coast With Awaiting Landing PartyДокумент2 страницыShips Near A Rocky Coast With Awaiting Landing PartyFouaAj1 FouaAj1Оценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Method Statement FINALДокумент61 страницаMethod Statement FINALshareyhou67% (3)
- Study and Interpretation of The ScoreДокумент10 страницStudy and Interpretation of The ScoreDwightPile-GrayОценок пока нет
- BarricadeДокумент6 страницBarricadeJithu PappachanОценок пока нет
- Landscape ArchitectureДокумент9 страницLandscape Architecturelisan2053Оценок пока нет
- 9701 Nos Ps 23Документ5 страниц9701 Nos Ps 23Hubbak KhanОценок пока нет
- Visi RuleДокумент6 страницVisi RuleBruce HerreraОценок пока нет
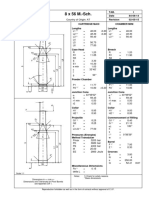
- 8 X 56 M.-SCH.: Country of Origin: ATДокумент1 страница8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimОценок пока нет
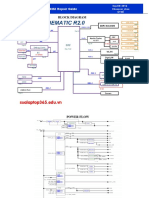
- Asus x453Документ5 страницAsus x453Rhiry Ntuh AthryОценок пока нет
- 6int 2008 Dec AДокумент6 страниц6int 2008 Dec ACharles_Leong_3417Оценок пока нет
- FluteДокумент13 страницFlutefisher3910% (1)
- 95-03097 Ballvlv300350 WCB PDFДокумент26 страниц95-03097 Ballvlv300350 WCB PDFasitdeyОценок пока нет
- Eng Notes2Документ10 страницEng Notes2Arti KapurОценок пока нет
- Chapter 5 - Principle of Marketing UpdateДокумент58 страницChapter 5 - Principle of Marketing UpdateKhaing HtooОценок пока нет
- Department of Education: Raiseplus Weekly Plan For Blended LearningДокумент3 страницыDepartment of Education: Raiseplus Weekly Plan For Blended LearningMARILYN CONSIGNAОценок пока нет
- Communication Skill - Time ManagementДокумент18 страницCommunication Skill - Time ManagementChấn NguyễnОценок пока нет
- The Original Lists of Persons of Quality Emigrants Religious Exiles Political Rebels Serving Men Sold For A Term of Years Apprentices Children Stolen Maidens Pressed and OthersДокумент609 страницThe Original Lists of Persons of Quality Emigrants Religious Exiles Political Rebels Serving Men Sold For A Term of Years Apprentices Children Stolen Maidens Pressed and OthersShakir Daddy-Phatstacks Cannon100% (1)
- Rdramirez Aota 2018 Poster For PortfolioДокумент1 страницаRdramirez Aota 2018 Poster For Portfolioapi-437843157Оценок пока нет
- Linux ProgramДокумент131 страницаLinux ProgramsivashaОценок пока нет
- SL Generator Ultrasunete RincoДокумент2 страницыSL Generator Ultrasunete RincoDariaОценок пока нет
- 4039-Texto Del Artículo-12948-3-10-20211123Документ14 страниц4039-Texto Del Artículo-12948-3-10-20211123Ricardo ApazaОценок пока нет
- You Can't Blame A FireДокумент8 страницYou Can't Blame A FireMontana QuarterlyОценок пока нет
- Thermodynamics WorksheetДокумент5 страницThermodynamics WorksheetMalcolmJustMalcolmОценок пока нет
- HangersSupportsReferenceDataGuide PDFДокумент57 страницHangersSupportsReferenceDataGuide PDFIndra RosadiОценок пока нет
- The Marriage of Figaro LibrettoДокумент64 страницыThe Marriage of Figaro LibrettoTristan BartonОценок пока нет
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет