Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- SAT Practice TestДокумент77 страницSAT Practice TestfhfsfplОценок пока нет
- Irina Maleeva - Ariel Snowflake x6 - ENG - FreeДокумент4 страницыIrina Maleeva - Ariel Snowflake x6 - ENG - FreeMarinaKorzinaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- PEAK Restoration of The Endodontically Treated ToothДокумент20 страницPEAK Restoration of The Endodontically Treated Toothlishenwong100% (1)
- Case Studies of Transportation Public-Private Partnerships Around The WorldДокумент158 страницCase Studies of Transportation Public-Private Partnerships Around The WorldzhenhuaruiОценок пока нет
- H107en 201906 r4 Elcor Elcorplus 20200903 Red1Документ228 страницH107en 201906 r4 Elcor Elcorplus 20200903 Red1mokbelОценок пока нет
- Treated ExfoliativeДокумент3 страницыTreated ExfoliativeaninuraniyahОценок пока нет
- Holstein Hargreaves Endo Topics 2003Документ11 страницHolstein Hargreaves Endo Topics 2003aninuraniyahОценок пока нет
- Holstein Hargreaves Endo Topics 2003Документ11 страницHolstein Hargreaves Endo Topics 2003aninuraniyahОценок пока нет
- PULPOTOMIДокумент8 страницPULPOTOMIaninuraniyahОценок пока нет
- Literatur 2Документ7 страницLiteratur 2aninuraniyahОценок пока нет
- 4 PDFДокумент3 страницы4 PDFLanggeng Perdhana Jangan MenyerahОценок пока нет
- Journal ReadingДокумент4 страницыJournal ReadingVeny AlfianiОценок пока нет
- MucoceleДокумент4 страницыMucoceleaninuraniyahОценок пока нет
- Systemic Diseases Caused by Oral InfectionДокумент12 страницSystemic Diseases Caused by Oral InfectionaninuraniyahОценок пока нет
- MucoceleДокумент4 страницыMucoceleaninuraniyahОценок пока нет
- Clinical Tips in Full Veneer Tooth Preparation: Review ArticleДокумент7 страницClinical Tips in Full Veneer Tooth Preparation: Review ArticleaninuraniyahОценок пока нет
- Global Handwashing Day 2013Документ2 страницыGlobal Handwashing Day 2013aninuraniyahОценок пока нет
- Journal ReadingДокумент4 страницыJournal ReadingVeny AlfianiОценок пока нет
- Eugenol 3Документ7 страницEugenol 3aninuraniyahОценок пока нет
- ExfoliativeДокумент4 страницыExfoliativeaninuraniyahОценок пока нет
- 4 PDFДокумент3 страницы4 PDFLanggeng Perdhana Jangan MenyerahОценок пока нет
- EugenolДокумент6 страницEugenolaninuraniyahОценок пока нет
- Eugenol 2Документ6 страницEugenol 2aninuraniyahОценок пока нет
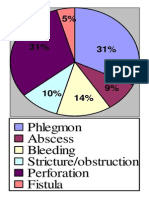
- Phlegmon Abscess Bleeding Stricture/obstruction Perforation FistulaДокумент1 страницаPhlegmon Abscess Bleeding Stricture/obstruction Perforation FistulaaninuraniyahОценок пока нет
- Ranula and Sublingual Salivary Gland ExcisionДокумент4 страницыRanula and Sublingual Salivary Gland ExcisionaninuraniyahОценок пока нет
- SterilisasiДокумент6 страницSterilisasianinuraniyahОценок пока нет
- Nursing Caries PedoДокумент37 страницNursing Caries PedoFourthMolar.comОценок пока нет
- 5-Surgical Treatment of RanulaДокумент5 страниц5-Surgical Treatment of RanulaDevi AlfianiОценок пока нет
- Gambaran Status KariesДокумент9 страницGambaran Status KariesaninuraniyahОценок пока нет
- Micro-Marsupialization Technique For Mucocele On Ventral Tongue in 4-Year-8-Month Old ChildДокумент2 страницыMicro-Marsupialization Technique For Mucocele On Ventral Tongue in 4-Year-8-Month Old ChildaninuraniyahОценок пока нет
- 90507414Документ5 страниц90507414aninuraniyahОценок пока нет
- Global Handwashing Day 2013Документ2 страницыGlobal Handwashing Day 2013aninuraniyahОценок пока нет
- Jop 2012 110716Документ8 страницJop 2012 110716aninuraniyahОценок пока нет
- Semi Finals in Tle 2015Документ3 страницыSemi Finals in Tle 2015LoraineTenorioОценок пока нет
- Math AA SL P 1 Marks SchemeДокумент6 страницMath AA SL P 1 Marks SchemeMrin GhoshОценок пока нет
- Potassium Fixation As Affected by Alternate Wetting and Drying in Some Soil Series of JharkhandДокумент4 страницыPotassium Fixation As Affected by Alternate Wetting and Drying in Some Soil Series of JharkhandDr Amrit Kumar JhaОценок пока нет
- FemДокумент4 страницыFemAditya SharmaОценок пока нет
- Passenger Lift Alert - Health and Safety AuthorityДокумент4 страницыPassenger Lift Alert - Health and Safety AuthorityReginald MaswanganyiОценок пока нет
- Lecture Planner - Inorganic Chemistry (Legend) - Yakeen NEET 2.0 2024Документ1 страницаLecture Planner - Inorganic Chemistry (Legend) - Yakeen NEET 2.0 2024Dipendra KumarОценок пока нет
- Rail Vehicle DynamicsДокумент55 страницRail Vehicle DynamicsdfОценок пока нет
- IV. Network Modeling, Simple SystemДокумент16 страницIV. Network Modeling, Simple SystemJaya BayuОценок пока нет
- CBSE DetailsДокумент6 страницCBSE DetailsNARESH KUMARОценок пока нет
- Tugas Dikumpulkan Pada Hari Sabtu, 11 April 2020. Apabila Email Bermasalah Dapat Mengirimkan Via WA PribadiДокумент4 страницыTugas Dikumpulkan Pada Hari Sabtu, 11 April 2020. Apabila Email Bermasalah Dapat Mengirimkan Via WA PribadiFebry SugiantaraОценок пока нет
- AKI in ChildrenДокумент43 страницыAKI in ChildrenYonas AwgichewОценок пока нет
- Mahindra & MahindraДокумент13 страницMahindra & MahindraAbhishek DharmadhikariОценок пока нет
- Lesson 1 Chapter 9 ErosiondepositionДокумент1 страницаLesson 1 Chapter 9 Erosiondepositionapi-249320969Оценок пока нет
- Fulltext 4 PDFДокумент4 страницыFulltext 4 PDFSubhadip Banerjee0% (1)
- Plastics and Polymer EngineeringДокумент4 страницыPlastics and Polymer Engineeringsuranjana26Оценок пока нет
- Determination of Drop-Impact Resistance of Plastic BottlesДокумент11 страницDetermination of Drop-Impact Resistance of Plastic BottlesAndres BrañaОценок пока нет
- Worksheet Series 5: Answer Any 3 Questions From 1 To 6. (2 Score Each)Документ6 страницWorksheet Series 5: Answer Any 3 Questions From 1 To 6. (2 Score Each)AswithОценок пока нет
- PIX4D Simply PowerfulДокумент43 страницыPIX4D Simply PowerfulJUAN BAQUEROОценок пока нет
- Electrowetting - Wikipedia, The Free EncyclopediaДокумент5 страницElectrowetting - Wikipedia, The Free EncyclopediaDwane AlmeidaОценок пока нет
- G.S 5Документ2 страницыG.S 5Jamsher BalochОценок пока нет
- AssessmentДокумент9 страницAssessmentJuan Miguel Sapad AlpañoОценок пока нет
- Reviews: The Global Epidemiology of HypertensionДокумент15 страницReviews: The Global Epidemiology of Hypertensionrifa iОценок пока нет
- Straight LineДокумент15 страницStraight LineAyanОценок пока нет
- Module 1 Notes The White Bird Reading The Image Painting Analysis PDFДокумент4 страницыModule 1 Notes The White Bird Reading The Image Painting Analysis PDFMelbely Rose Apigo BaduaОценок пока нет
- Lafarge Interior Building Solutions BrochureДокумент24 страницыLafarge Interior Building Solutions BrochuretwinpixtwinpixОценок пока нет
- Syllabus Unit Iv Unit Commitment and Economic DispatchДокумент23 страницыSyllabus Unit Iv Unit Commitment and Economic DispatchBALAKRISHNANОценок пока нет