Вам также может понравиться
- Research Article Plasma Fibrin Clot Properties As Determinants of Bleeding Time in Human Subjects: Association With Histidine-Rich GlycoproteinДокумент11 страницResearch Article Plasma Fibrin Clot Properties As Determinants of Bleeding Time in Human Subjects: Association With Histidine-Rich GlycoproteinAyu Nabila Kusuma PradanaОценок пока нет
- Maternity Hospital Bag Checklist PDFДокумент1 страницаMaternity Hospital Bag Checklist PDFAyu Nabila Kusuma PradanaОценок пока нет
- Jurnal Kulit Ayu 5Документ2 страницыJurnal Kulit Ayu 5Ayu Nabila Kusuma PradanaОценок пока нет
- Journal Pone 0104375Документ7 страницJournal Pone 0104375Ayu Nabila Kusuma PradanaОценок пока нет
- Rabu, 1 Juli 2015 06:00 WIB S/D Kamis, 2 Juli 2015 Pk. 06:00 WIBДокумент23 страницыRabu, 1 Juli 2015 06:00 WIB S/D Kamis, 2 Juli 2015 Pk. 06:00 WIBAyu Nabila Kusuma PradanaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Acid Base Electolytes QuestionsДокумент4 страницыAcid Base Electolytes QuestionsDonna R. Joyce0% (1)
- Therapeutics in Endodontics: DR Mohamed RabieДокумент75 страницTherapeutics in Endodontics: DR Mohamed RabieAbdelrahman GalalОценок пока нет
- NDC LA - AmerigroupДокумент5 страницNDC LA - Amerigroupkarts23Оценок пока нет
- A 20 Year Old Man Suffered From A Spinal Cord Injury at The C2 To C3 Level As The Result of A Motorcycle AccidentДокумент4 страницыA 20 Year Old Man Suffered From A Spinal Cord Injury at The C2 To C3 Level As The Result of A Motorcycle AccidentqingwenОценок пока нет
- Zentel Tablets: What Is in This LeafletДокумент3 страницыZentel Tablets: What Is in This LeafletLadyKahluaОценок пока нет
- health care system of swedenبДокумент34 страницыhealth care system of swedenبAhmedAljebouli0% (1)
- The Tylenol Crisis: How Effective Public Relations Saved Johnson & JohnsonДокумент7 страницThe Tylenol Crisis: How Effective Public Relations Saved Johnson & Johnsonchocobearsweets100% (1)
- Phenytoin Drug StudyДокумент3 страницыPhenytoin Drug StudyCheezy Bread100% (1)
- Drugs That Require Frequent MonitoringДокумент22 страницыDrugs That Require Frequent MonitoringNader Smadi100% (7)
- Kuantitas Obat Tahun NewДокумент18 страницKuantitas Obat Tahun NewFathia Afriza KurniawatiОценок пока нет
- Classification of DrugsДокумент15 страницClassification of DrugsAwani OОценок пока нет
- Algorithm Hypertension Sci PDFДокумент1 страницаAlgorithm Hypertension Sci PDFGustavo CabanasОценок пока нет
- Incepta Pharmaceuticals LTD Bangladesh Products ListДокумент35 страницIncepta Pharmaceuticals LTD Bangladesh Products Listelectryfing asif82% (11)
- Cream & SalepДокумент6 страницCream & SalepDesti WulandariОценок пока нет
- Medication Conversion ChartДокумент2 страницыMedication Conversion ChartIlinca mirnoviciОценок пока нет
- TGP Luzon SRP - PDF Nov 27Документ14 страницTGP Luzon SRP - PDF Nov 27Hatingmewont Keepyoupretty100% (1)
- 1 Laporan Pengeluaran Obat Dan Alkes Depyan 28 SEPTEMBER 2019Документ18 страниц1 Laporan Pengeluaran Obat Dan Alkes Depyan 28 SEPTEMBER 2019Indah SetyowatiОценок пока нет
- MorphineДокумент13 страницMorphineNajihah Izzah100% (2)
- BAD Specials BookletДокумент12 страницBAD Specials BookletzfjasimОценок пока нет
- Community Pharmacy Practice in PakistanДокумент18 страницCommunity Pharmacy Practice in Pakistanthundercat123Оценок пока нет
- Bek Kelompok 1Документ19 страницBek Kelompok 1kiranaОценок пока нет
- Aparato 3 USP DisoluciónДокумент5 страницAparato 3 USP Disoluciónalejandro elizaldeОценок пока нет
- SH0512Документ12 страницSH0512Anonymous 9eadjPSJNgОценок пока нет
- Psychiatric MedicationДокумент22 страницыPsychiatric MedicationSofia Centro TaerОценок пока нет
- Data Pasien Potensi PRB Jan-Juni 2019Документ212 страницData Pasien Potensi PRB Jan-Juni 2019Adra AdeОценок пока нет
- Co-Pay Rise To Hurt Indigenous: Guardian Picks Up Satisfaction Award 9,062 Meds EnquiriesДокумент2 страницыCo-Pay Rise To Hurt Indigenous: Guardian Picks Up Satisfaction Award 9,062 Meds EnquiriespharmacydailyОценок пока нет
- Drugs MnemonicsДокумент6 страницDrugs MnemonicsDarrylJavier100% (1)
- Drug Deaths in Jefferson County 2015Документ16 страницDrug Deaths in Jefferson County 2015Jeremy W. Gray100% (1)
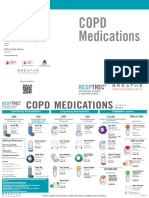
- Courses Offered:: Copd MedicationsДокумент2 страницыCourses Offered:: Copd MedicationsDave BoyОценок пока нет
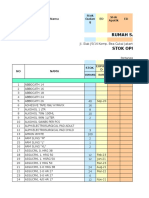
- Stock Opname Bulan September 2018Документ138 страницStock Opname Bulan September 2018Miftah RamadhanОценок пока нет