Вам также может понравиться
- Abortion rights- a matter of human rights and social justiceДокумент7 страницAbortion rights- a matter of human rights and social justiceMohammed ShahbazОценок пока нет
- Topic 12 - Madhumayanti - 190701224political ScienceДокумент7 страницTopic 12 - Madhumayanti - 190701224political ScienceMadhumayanti NandiОценок пока нет
- Medical Termination of Pregnancy Act 1971Документ24 страницыMedical Termination of Pregnancy Act 1971ramshaОценок пока нет
- Research On Illegal Termination of PregnancyДокумент17 страницResearch On Illegal Termination of PregnancyRajeev shuklaОценок пока нет
- Right To AbortionДокумент14 страницRight To AbortionSanjay .GОценок пока нет
- Chapter 1 - Introduction: A Study of Women's Right To Abort Under The Indian Legal FrameworkДокумент9 страницChapter 1 - Introduction: A Study of Women's Right To Abort Under The Indian Legal FrameworkSaket RaoОценок пока нет
- IHL - 11A024 and 11B144 ProjectДокумент17 страницIHL - 11A024 and 11B144 ProjectShubham PhophaliaОценок пока нет
- Jamia Millia Islamia University Faculty of LawДокумент22 страницыJamia Millia Islamia University Faculty of LawTaiyabaОценок пока нет
- Abortion RightДокумент4 страницыAbortion RightAman MishraОценок пока нет
- FinalДокумент45 страницFinalRanvidsОценок пока нет
- Family Law ProjectДокумент16 страницFamily Law ProjectSarthak ChaudharyОценок пока нет
- Mother and The Fetus: A Socio-Legal Conflict: Ms - Asween KaurДокумент14 страницMother and The Fetus: A Socio-Legal Conflict: Ms - Asween KaurShakshi MehtaОценок пока нет
- Health Law - AzeemДокумент34 страницыHealth Law - AzeemMohd AqibОценок пока нет
- Abortion Laws in IndiaДокумент7 страницAbortion Laws in IndiaVaishnavi ParateОценок пока нет
- Chanakya National Law University, Patna: Health Law Project On: Abortion Rights: A Global PerspectiveДокумент52 страницыChanakya National Law University, Patna: Health Law Project On: Abortion Rights: A Global PerspectiveRanvidsОценок пока нет
- Abortion Law in IndiaДокумент12 страницAbortion Law in IndiaRajwinder KaurОценок пока нет
- Class Seminar: Army Institute of Law, MohaliДокумент13 страницClass Seminar: Army Institute of Law, Mohalimridu aroraОценок пока нет
- Research Paper Panjab University Law Review,: Shweta DhirДокумент8 страницResearch Paper Panjab University Law Review,: Shweta Dhirswati vermaОценок пока нет
- 14 - Research Papers PDFДокумент8 страниц14 - Research Papers PDFswati vermaОценок пока нет
- Medical Termination of Pregnancy Act - IpleadersДокумент25 страницMedical Termination of Pregnancy Act - IpleadersSoumya Ranjan BarikОценок пока нет
- Abortion Laws in IndiaДокумент9 страницAbortion Laws in IndiaImran KhanОценок пока нет
- Health Law-Final AnswerДокумент35 страницHealth Law-Final AnswerShashwat PathakОценок пока нет
- Surprise Test of Health LawДокумент11 страницSurprise Test of Health LawkhanОценок пока нет
- Surprise Test of Health LawДокумент11 страницSurprise Test of Health LawsamirОценок пока нет
- Laws Related To Miscarriage of Foetus in The Womb in IndiaДокумент8 страницLaws Related To Miscarriage of Foetus in The Womb in IndiaAdarsh ShetОценок пока нет
- Termination of PregnancyДокумент7 страницTermination of PregnancyragyaОценок пока нет
- 2017-12 Comparative Constitutional LawДокумент9 страниц2017-12 Comparative Constitutional LawMayank TripathiОценок пока нет
- Right To Health in India - Comtemporary Issues and Concerns - Dr. Abhijit DasДокумент21 страницаRight To Health in India - Comtemporary Issues and Concerns - Dr. Abhijit Dasrajnish2555Оценок пока нет
- Sai Abhipsa Gochhayat: Understanding of Right To Abortion Under Indian ConstitutionДокумент10 страницSai Abhipsa Gochhayat: Understanding of Right To Abortion Under Indian ConstitutionMalaisamy AОценок пока нет
- Research Paper On Right To Life of A FoetusДокумент5 страницResearch Paper On Right To Life of A FoetusRaghav GuptaОценок пока нет
- Arguments As To Why This Bill Should Be PassedДокумент21 страницаArguments As To Why This Bill Should Be Passedrotsacrreijav123Оценок пока нет
- Health Law Exam - Anas MohsinДокумент44 страницыHealth Law Exam - Anas MohsinMohd AqibОценок пока нет
- Petitioners: James M. Imbong and LovelyДокумент3 страницыPetitioners: James M. Imbong and LovelyKang MinheeОценок пока нет
- Abortion (Se)Документ6 страницAbortion (Se)Shanty RosianaОценок пока нет
- Memorials Respondent1.1Документ13 страницMemorials Respondent1.1Pavan KumarОценок пока нет
- RH Law g10Документ68 страницRH Law g10Alfin Jeffbrice BengueloОценок пока нет
- Law Relating To Human Rights Final DraftДокумент36 страницLaw Relating To Human Rights Final DraftAnwesha TripathyОценок пока нет
- Assignment - 405Документ7 страницAssignment - 405achal.yadav125Оценок пока нет
- Document (21) .Документ9 страницDocument (21) .NaveedОценок пока нет
- Legalization Abortion in IndiaДокумент13 страницLegalization Abortion in IndiaNeetish Kumar HandaОценок пока нет
- Law N Et Unit 3 and 4Документ160 страницLaw N Et Unit 3 and 4Vaibhav SinghОценок пока нет
- WOMEN AND LAW PSDA ON - Google DocsДокумент8 страницWOMEN AND LAW PSDA ON - Google DocsRheaОценок пока нет
- Health NotesДокумент36 страницHealth NotesTANISHA PRASADОценок пока нет
- SocioДокумент9 страницSocioElena ZareОценок пока нет
- AbortionДокумент11 страницAbortionKopal GargОценок пока нет
- RA 10354, Also Known As "The Responsible Parenthood and Reproductive Health Act of 2012", HasДокумент9 страницRA 10354, Also Known As "The Responsible Parenthood and Reproductive Health Act of 2012", HascianОценок пока нет
- Ethical Issues Pertaining To AbortionДокумент38 страницEthical Issues Pertaining To AbortionRoman MamunОценок пока нет
- Women's Right to Abortion Under International LawДокумент10 страницWomen's Right to Abortion Under International LawFayeОценок пока нет
- RH Law 2Документ17 страницRH Law 2Davie PascuaОценок пока нет
- Abhishek ArticleДокумент5 страницAbhishek Articledhruv sharmaОценок пока нет
- S S L G: Aipur Ational NiversityДокумент32 страницыS S L G: Aipur Ational NiversitySapna KawatОценок пока нет
- Medical TerminationДокумент14 страницMedical TerminationNagarjun GowdaОценок пока нет
- Women's Rights to Equality, Autonomy and Reproductive HealthДокумент8 страницWomen's Rights to Equality, Autonomy and Reproductive HealthJustina MačiulytėОценок пока нет
- Kenya's Complex Abortion DebateДокумент13 страницKenya's Complex Abortion DebateNjokiОценок пока нет
- Rule 20Документ16 страницRule 20Noel SihОценок пока нет
- Rule 20 Precautionary PrincipleДокумент53 страницыRule 20 Precautionary PrinciplesakuraОценок пока нет
- Right To HealthДокумент3 страницыRight To HealthHiranmaya NandaОценок пока нет
- Rule 20 Precautionary Principle in Imbong v OchoaДокумент53 страницыRule 20 Precautionary Principle in Imbong v OchoasakuraОценок пока нет
- Imbong Vs Ochoa Case DigestДокумент15 страницImbong Vs Ochoa Case DigestBenedick LedesmaОценок пока нет
- Form 8: Application For Correction To Particulars Entered in Electoral RollДокумент10 страницForm 8: Application For Correction To Particulars Entered in Electoral RollAnonymous tOgAKZ8Оценок пока нет
- Protection of Refugees in IndiaДокумент10 страницProtection of Refugees in IndiaSameer KhanОценок пока нет
- Sharique Raza - LawДокумент3 страницыSharique Raza - LawAnonymous tOgAKZ8Оценок пока нет
- Assignment On Specific Groups (DR Nazia Khan)Документ25 страницAssignment On Specific Groups (DR Nazia Khan)Anonymous tOgAKZ8Оценок пока нет
- Uttrakhand GK Pariksha Vani Part-I@Документ84 страницыUttrakhand GK Pariksha Vani Part-I@Anonymous tOgAKZ8Оценок пока нет
- ApplicationДокумент1 страницаApplicationAnonymous tOgAKZ8Оценок пока нет
- AffidavitonRs 10StampPaperДокумент1 страницаAffidavitonRs 10StampPaperAnonymous tOgAKZ8Оценок пока нет
- Disaster Management Report: Types, Issues & ManagementДокумент22 страницыDisaster Management Report: Types, Issues & ManagementAnonymous tOgAKZ8Оценок пока нет
- Types of Quantitative Research Methods-1Документ16 страницTypes of Quantitative Research Methods-1MuhammadShahzebОценок пока нет
- Rights of Disabled Persons Project ReportДокумент25 страницRights of Disabled Persons Project ReportAnonymous tOgAKZ8Оценок пока нет
- Evolution of International OrganisationsДокумент13 страницEvolution of International OrganisationsDr. Afroz Alam88% (26)
- Assignment On Science and Technology (Bulbur Dhar)Документ11 страницAssignment On Science and Technology (Bulbur Dhar)Anonymous tOgAKZ8Оценок пока нет
- Bushra ApplicationДокумент1 страницаBushra ApplicationAnonymous tOgAKZ8Оценок пока нет
- Bushra ApplicationДокумент1 страницаBushra ApplicationAnonymous tOgAKZ8Оценок пока нет
- Evolution of International OrganisationsДокумент13 страницEvolution of International OrganisationsDr. Afroz Alam88% (26)
- ApplicationДокумент1 страницаApplicationAnonymous tOgAKZ8Оценок пока нет
- Qualitative Research: Name: Mohd Amerul Akmal Bin Mohd Yunos: Syahidani Binti Mohamed: Nabilah Faiqah Binti AzmanДокумент11 страницQualitative Research: Name: Mohd Amerul Akmal Bin Mohd Yunos: Syahidani Binti Mohamed: Nabilah Faiqah Binti AzmanAnonymous tOgAKZ8Оценок пока нет
- Assignment On International OrgansationДокумент15 страницAssignment On International OrgansationAnonymous tOgAKZ8Оценок пока нет
- Uttrakhand GK Pariksha Vani Part-I@Документ84 страницыUttrakhand GK Pariksha Vani Part-I@Anonymous tOgAKZ8Оценок пока нет
- Vice Commission: Haryana Public Service Commission HCS (Judicial Branch) Preliminary Examination - 2020-21Документ1 страницаVice Commission: Haryana Public Service Commission HCS (Judicial Branch) Preliminary Examination - 2020-21Anonymous tOgAKZ8Оценок пока нет
- Sharique Nai UdaanДокумент1 страницаSharique Nai UdaanAnonymous tOgAKZ8Оценок пока нет
- Utrakhand Apo SyllabusДокумент3 страницыUtrakhand Apo SyllabusAnonymous tOgAKZ8Оценок пока нет
- Human ColoningДокумент15 страницHuman ColoningAnonymous tOgAKZ8Оценок пока нет
- Self Declaration of Minority Community by StudentsДокумент1 страницаSelf Declaration of Minority Community by StudentsAnonymous tOgAKZ8Оценок пока нет
- Vice Commission: Haryana Public Service Commission HCS (Judicial Branch) Preliminary Examination - 2020-21Документ1 страницаVice Commission: Haryana Public Service Commission HCS (Judicial Branch) Preliminary Examination - 2020-21Anonymous tOgAKZ8Оценок пока нет
- ApplicationДокумент1 страницаApplicationAnonymous tOgAKZ8Оценок пока нет
- Sharique Nai UdaanДокумент1 страницаSharique Nai UdaanAnonymous tOgAKZ8Оценок пока нет
- Assignment On International OrgansationДокумент15 страницAssignment On International OrgansationAnonymous tOgAKZ8Оценок пока нет
- Assignment On Science and Technology (Bulbur Dhar)Документ11 страницAssignment On Science and Technology (Bulbur Dhar)Anonymous tOgAKZ8Оценок пока нет
- Hera GovernaceДокумент13 страницHera GovernaceAnonymous tOgAKZ8Оценок пока нет
- Overhead Set (OBC)Документ19 страницOverhead Set (OBC)MohamedОценок пока нет
- The Bresle Method: Improving Accuracy of Soluble Salt MeasurementsДокумент4 страницыThe Bresle Method: Improving Accuracy of Soluble Salt MeasurementsMuthuKumarОценок пока нет
- Jamec Air FittingsДокумент18 страницJamec Air Fittingsgoeez1Оценок пока нет
- Indian Boyhood PDFДокумент316 страницIndian Boyhood PDFHasanОценок пока нет
- Evolution Chart 3Документ1 страницаEvolution Chart 3sasupraОценок пока нет
- Electrolyte AE 11 - MSDSДокумент8 страницElectrolyte AE 11 - MSDSShinta Nugraha MughniОценок пока нет
- Class9. CVD and PVDДокумент30 страницClass9. CVD and PVDiraОценок пока нет
- VERALLIA WHITE-BOOK EN March2022 PDFДокумент48 страницVERALLIA WHITE-BOOK EN March2022 PDFEugenio94Оценок пока нет
- Eltra Cs 530Документ122 страницыEltra Cs 530ahalonsoОценок пока нет
- Borri Ups b9000 Ups Service Manual - CompressДокумент180 страницBorri Ups b9000 Ups Service Manual - CompressArun SОценок пока нет
- Small Gas Turbines 4 LubricationДокумент19 страницSmall Gas Turbines 4 LubricationValBMSОценок пока нет
- Nursing Care of ElderlyДокумент26 страницNursing Care of ElderlyIndra KumarОценок пока нет
- INFORSHT Produktkatalog en Web 03.22Документ13 страницINFORSHT Produktkatalog en Web 03.22lolОценок пока нет
- Specialized Connective TissueДокумент15 страницSpecialized Connective TissueSebОценок пока нет
- EDSP Quantitative and Qualitative FormДокумент2 страницыEDSP Quantitative and Qualitative FormTalal SultanОценок пока нет
- Berman Et Al-2019-Nature Human BehaviourДокумент5 страницBerman Et Al-2019-Nature Human BehaviourMira mОценок пока нет
- El Bill PDFДокумент2 страницыEl Bill PDFvinodОценок пока нет
- Persuasive Essay Eng 101nДокумент6 страницPersuasive Essay Eng 101napi-341545248Оценок пока нет
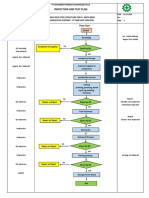
- Inspection and Test Plan: Flow Chart Start IncomingДокумент1 страницаInspection and Test Plan: Flow Chart Start IncomingSinden AyuОценок пока нет
- GDCR Final PDFДокумент311 страницGDCR Final PDFHrushikesh PatelОценок пока нет
- Accuracy of Real-Time Shear Wave Elastography in SДокумент10 страницAccuracy of Real-Time Shear Wave Elastography in SApotik ApotekОценок пока нет
- Reflective Essay Assignment #8 - Managing Emotions and Coping With StressДокумент2 страницыReflective Essay Assignment #8 - Managing Emotions and Coping With StressRej GarbosaОценок пока нет
- CSK - W - My - Mother - at - Sixty - Six 2Документ2 страницыCSK - W - My - Mother - at - Sixty - Six 2Aaron JoshiОценок пока нет
- Chambal Cable Stayed Bridge Connecting ShoresДокумент6 страницChambal Cable Stayed Bridge Connecting Shoresafzal taiОценок пока нет
- Coal Workers' Pneumoconiosis (Black Lung Disease) Treatment & Management - Approach Considerations, Medical Care, Surgical CareДокумент2 страницыCoal Workers' Pneumoconiosis (Black Lung Disease) Treatment & Management - Approach Considerations, Medical Care, Surgical CareامينОценок пока нет
- Restaurant Supervisor Job Description Job SummaryДокумент3 страницыRestaurant Supervisor Job Description Job SummaryKumarSvОценок пока нет
- Sugar Reseach in AustraliaДокумент16 страницSugar Reseach in AustraliaJhonattanIsaacОценок пока нет
- The Truth About EtawahДокумент4 страницыThe Truth About EtawahPoojaDasgupta100% (1)
- Recombinant DNA TechnologyДокумент14 страницRecombinant DNA TechnologyAnshika SinghОценок пока нет
- Research PaperДокумент12 страницResearch PapershreyanshОценок пока нет