Вам также может понравиться
- Claw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandClaw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsРейтинг: 4 из 5 звезд4/5 (1)
- The Thoracic Outlet Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandThe Thoracic Outlet Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- F - Proximal Ulnar Nerve Injury Correct AnswerДокумент26 страницF - Proximal Ulnar Nerve Injury Correct AnswerMehdi Hasan MazumderОценок пока нет
- Forearm fractures and wrist injuriesДокумент1 страницаForearm fractures and wrist injuriesintan rosliОценок пока нет
- Orthopedic SlidesДокумент78 страницOrthopedic SlidesAzry Mustapa100% (1)
- Acetabular Fracture PostgraduateДокумент47 страницAcetabular Fracture Postgraduatekhalidelsir5100% (1)
- Median Nerve Injury Causes Ape Hand DeformityДокумент16 страницMedian Nerve Injury Causes Ape Hand Deformitymedical- physio classesОценок пока нет
- M.S. Orthopaedic Surgery SyllabusДокумент8 страницM.S. Orthopaedic Surgery SyllabusMuthu KumarОценок пока нет
- Biomechanics of The ElbowДокумент16 страницBiomechanics of The ElbowAsmaa Ahmad SharawyОценок пока нет
- Hip ExaminationДокумент84 страницыHip ExaminationDeepak KumarОценок пока нет
- Spinal Cord InjuryДокумент39 страницSpinal Cord InjuryrahatОценок пока нет
- Upper Limb Orthosis - Dr. Bhaskarananda KumarДокумент33 страницыUpper Limb Orthosis - Dr. Bhaskarananda KumarsudiptomukherjeeОценок пока нет
- UKA: When Would I Do It?Документ35 страницUKA: When Would I Do It?neareastspineОценок пока нет
- Ficat and Arlet staging of hip AVNДокумент6 страницFicat and Arlet staging of hip AVNFernando Sugiarto0% (1)
- Examining Peripheral NervesДокумент6 страницExamining Peripheral NervesNur Atiqah ZainalОценок пока нет
- Spine: HistoryДокумент6 страницSpine: HistorySham SundarОценок пока нет
- Spine Fractures and Spinal Cord InjuryДокумент54 страницыSpine Fractures and Spinal Cord InjuryAloy PudeОценок пока нет
- Spine Examination: Mario Johan Heryputra 11.2012.208Документ29 страницSpine Examination: Mario Johan Heryputra 11.2012.208Mario Johan Heryputra100% (1)
- Rehabilitation of Cerebral Palsy & Motor DelayДокумент49 страницRehabilitation of Cerebral Palsy & Motor DelayasloocltОценок пока нет
- Why Every Spine Fusion Can Be A Deformity?Документ88 страницWhy Every Spine Fusion Can Be A Deformity?PaulMcAfeeОценок пока нет
- Tendon TransferДокумент1 страницаTendon TransferPandi Smart VjОценок пока нет
- Diseases of The Spinal CordДокумент89 страницDiseases of The Spinal CordLolla SinwarОценок пока нет
- Orthopedic InjuriesДокумент27 страницOrthopedic InjuriesvikramОценок пока нет
- Elbow Special TestДокумент4 страницыElbow Special TestEllaiza Astacaan100% (1)
- Cardio Pulmonary AssessmentДокумент8 страницCardio Pulmonary AssessmentSHAIK SHABEENAОценок пока нет
- CTEVДокумент25 страницCTEVIceBearОценок пока нет
- Orthopedic SurgeryДокумент53 страницыOrthopedic SurgeryGeorgeОценок пока нет
- Bicipital TendonitisДокумент2 страницыBicipital TendonitisJ Cheung100% (2)
- Forearm & Hand AnatomyДокумент5 страницForearm & Hand AnatomyshivnairОценок пока нет
- Approach To FractureДокумент17 страницApproach To FractureRebecca WongОценок пока нет
- Orthopedic EquipmentsДокумент14 страницOrthopedic Equipmentsdavid_soОценок пока нет
- Disability Evaluation: Radhika ChintamaniДокумент58 страницDisability Evaluation: Radhika ChintamaniBhavya Amin0% (1)
- Amc Limb FractureДокумент10 страницAmc Limb Fractureffaa100% (1)
- Cerebral Palsy Revalida FormatДокумент10 страницCerebral Palsy Revalida FormatChelsea CalanoОценок пока нет
- Nerves of Upper Limb and Their Injuries: Learning ObjectivesДокумент11 страницNerves of Upper Limb and Their Injuries: Learning ObjectivesRumana AliОценок пока нет
- Carpal Tunnel Syndrome FinalДокумент4 страницыCarpal Tunnel Syndrome Finalcatherine_suganob6496100% (2)
- Neurological ExaminationДокумент32 страницыNeurological ExaminationJuling PeralesОценок пока нет
- Neurological ExaminationДокумент13 страницNeurological Examinationsaveetha purushothamanОценок пока нет
- Ankel Heel PainДокумент51 страницаAnkel Heel PainMeno Ali100% (1)
- Juvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDДокумент38 страницJuvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDLavi GoyalОценок пока нет
- Hip Dislocation Reduction ManueverДокумент6 страницHip Dislocation Reduction ManueverAdam IrsyaddyraОценок пока нет
- Rare spinal cord disease syringomyelia definition causes symptoms treatmentДокумент8 страницRare spinal cord disease syringomyelia definition causes symptoms treatmentNurfadiyah YasinОценок пока нет
- RS2480 Amputation 2018Документ49 страницRS2480 Amputation 2018Hung Sarah100% (1)
- Principles of Tendon Transfer in The Hand and ForearmДокумент9 страницPrinciples of Tendon Transfer in The Hand and Forearm'Ema Surya PertiwiОценок пока нет
- JBLMRH - Ortho - Lag Screw TechniqueДокумент17 страницJBLMRH - Ortho - Lag Screw TechniqueTristan ArellanoОценок пока нет
- Spinal Cord Injury, DisordersДокумент54 страницыSpinal Cord Injury, DisordersChananОценок пока нет
- Neuro AssessmentДокумент23 страницыNeuro AssessmentSidra aliОценок пока нет
- Diseases of Spine andДокумент37 страницDiseases of Spine andgunawan djayaОценок пока нет
- Shoulder Dislocation DraftДокумент26 страницShoulder Dislocation Drafthusnajihah18Оценок пока нет
- Soft tissue injury treatment RICEДокумент2 страницыSoft tissue injury treatment RICEDenis Edem Dzebre100% (1)
- Cranial NervesДокумент16 страницCranial Nervesapi-302547403100% (1)
- Gpe - 017.1 - Orthopaedic ExaminationДокумент3 страницыGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumОценок пока нет
- Spinal Cord Injuries: Gabriel C. Tender, MDДокумент49 страницSpinal Cord Injuries: Gabriel C. Tender, MDCathyCarltonОценок пока нет
- Peripheral Nerve Examination (Final)Документ2 страницыPeripheral Nerve Examination (Final)Nurul Amalina OsmanОценок пока нет
- Elbow Complex (Kinesiology)Документ2 страницыElbow Complex (Kinesiology)Kimmybee Garcia50% (2)
- The Trunk and Spinal ColumnДокумент41 страницаThe Trunk and Spinal Columnrex100% (1)
- Basic Chest X-Ray Interpretation (5minutes Talk) : DR - Alemayehu (ECCM R1)Документ35 страницBasic Chest X-Ray Interpretation (5minutes Talk) : DR - Alemayehu (ECCM R1)Alex beharuОценок пока нет
- TARGET 200 PLUS Orthopaedics GuideДокумент21 страницаTARGET 200 PLUS Orthopaedics GuideTMC PGI GENER MICKOОценок пока нет
- DR - O. K. A. SamuelsДокумент76 страницDR - O. K. A. Samuelsgdudex118811Оценок пока нет
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsРейтинг: 4 из 5 звезд4/5 (2)
- Urology MCQsДокумент13 страницUrology MCQsRahmah Shah Bahai83% (6)
- Head and Neck SurgeryДокумент2 страницыHead and Neck SurgeryRahmah Shah BahaiОценок пока нет
- TraumaДокумент5 страницTraumaRahmah Shah BahaiОценок пока нет
- EMQs in SurgeryДокумент25 страницEMQs in Surgerynob2011nob100% (2)
- Hernia & Abdominal WallДокумент2 страницыHernia & Abdominal WallRahmah Shah BahaiОценок пока нет
- Cushing's SyndromeДокумент25 страницCushing's SyndromeRahmah Shah BahaiОценок пока нет
- TransplantationДокумент1 страницаTransplantationRahmah Shah BahaiОценок пока нет
- Saudi Board Exam - Surgery Questions from 2009 Exam (192/200Документ47 страницSaudi Board Exam - Surgery Questions from 2009 Exam (192/200Rahmah Shah Bahai100% (2)
- Head and Neck SurgeryДокумент2 страницыHead and Neck SurgeryRahmah Shah BahaiОценок пока нет
- Saudi Board Exam - Surgery Questions from 2009 Exam (192/200Документ47 страницSaudi Board Exam - Surgery Questions from 2009 Exam (192/200Rahmah Shah Bahai100% (2)
- كتيب البرنامج - الجراحة العامة الزمالة السعوديةДокумент124 страницыكتيب البرنامج - الجراحة العامة الزمالة السعوديةRahmah Shah BahaiОценок пока нет
- 1st Part Arab Board Exam in General Surgery, June 2007Документ18 страниц1st Part Arab Board Exam in General Surgery, June 2007Rahmah Shah Bahai50% (4)
- VVI Hypothyroidism For PresntationДокумент12 страницVVI Hypothyroidism For PresntationRahmah Shah BahaiОценок пока нет
- Day Designer Daily Page Final - Copyright - Do Not DistributeДокумент1 страницаDay Designer Daily Page Final - Copyright - Do Not DistributelauveromОценок пока нет
- Pediatrics 2006 Congenital Hypothyroidism GuidelinesДокумент16 страницPediatrics 2006 Congenital Hypothyroidism GuidelinesRahmah Shah BahaiОценок пока нет
- Ped Adrenal InsufficiencyДокумент13 страницPed Adrenal InsufficiencyRahmah Shah BahaiОценок пока нет
- Ped Obesity Flip Chart AAPДокумент24 страницыPed Obesity Flip Chart AAPRahmah Shah BahaiОценок пока нет
- AAFP-Short and Tall StatureДокумент8 страницAAFP-Short and Tall StatureRahmah Shah BahaiОценок пока нет
- Hypocalcemia CasesДокумент4 страницыHypocalcemia CasesRahmah Shah BahaiОценок пока нет
- Supervised by Dr. Najlaa JassasДокумент29 страницSupervised by Dr. Najlaa JassasRahmah Shah BahaiОценок пока нет
- Cerebral Palsy CPДокумент59 страницCerebral Palsy CPRahmah Shah BahaiОценок пока нет
- Anatomy One Shot DR AshwiniДокумент95 страницAnatomy One Shot DR Ashwinienthusiast383Оценок пока нет
- The Basics of ElectromyographyДокумент4 страницыThe Basics of ElectromyographyCamila MendezОценок пока нет
- Orthopedics McqsДокумент34 страницыOrthopedics McqsMadhu Sudhan Pandeya100% (1)
- Dissection Notes: Upper Limb MusclesДокумент42 страницыDissection Notes: Upper Limb MusclesGeoffreyОценок пока нет
- Borders of The Cubital FossaДокумент2 страницыBorders of The Cubital FossaSweäta DasОценок пока нет
- Biceps Brachii OriginДокумент40 страницBiceps Brachii OriginDanish GujjarОценок пока нет
- Paces 7 - Cns - Upper LimbДокумент11 страницPaces 7 - Cns - Upper LimbDrShamshad KhanОценок пока нет
- LP needle structure lumbar punctureДокумент92 страницыLP needle structure lumbar punctureJohn M. Hemsworth100% (1)
- Compa Horse and Human - NervesДокумент12 страницCompa Horse and Human - NervesJames SumagaysayОценок пока нет
- Yuxing Liu - Wrist and Ankle AcupunctureДокумент40 страницYuxing Liu - Wrist and Ankle AcupunctureHaryono zhu100% (1)
- Anatomy Solved Papers 2009 To 2013Документ35 страницAnatomy Solved Papers 2009 To 2013Lakshmi Venkataraman90% (10)
- Hydrodissection of Peripheral Nerve EntrapmentsДокумент7 страницHydrodissection of Peripheral Nerve Entrapmentsadam.stenmanОценок пока нет
- S17 BL Shoulder and Brachial Plexus 21Документ39 страницS17 BL Shoulder and Brachial Plexus 212110052 BRYAN RICARDO HANDOKOОценок пока нет
- A. Transverse Ligament: B. Ligamentum TeresДокумент30 страницA. Transverse Ligament: B. Ligamentum TeresUsmle seekerОценок пока нет
- Orthopaedic Surgery CritiquesДокумент16 страницOrthopaedic Surgery CritiquesAlvand HormoziОценок пока нет
- Muscles of Upper LimbДокумент21 страницаMuscles of Upper Limbمحمد علىОценок пока нет
- Recent Questions 2019 Section AДокумент87 страницRecent Questions 2019 Section ASuresh ChevagoniОценок пока нет
- Blood Supply of Upper LimbДокумент35 страницBlood Supply of Upper LimbfdjkvfjvОценок пока нет
- Radial Nerve PalsyДокумент10 страницRadial Nerve Palsycemm_11Оценок пока нет
- Feigl 2020Документ8 страницFeigl 2020eralp cevikkalpОценок пока нет
- Anatomy Review of Extreme TiesДокумент65 страницAnatomy Review of Extreme Tiesskihard0404749Оценок пока нет
- Muscles of the Pectoral Region and BackДокумент9 страницMuscles of the Pectoral Region and Backshananana1616Оценок пока нет
- Muscle Innervation Chart IIДокумент7 страницMuscle Innervation Chart IIkimsue9448Оценок пока нет
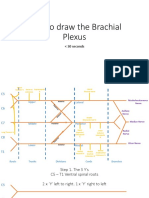
- How To Draw The Brachial PlexusДокумент16 страницHow To Draw The Brachial PlexusHОценок пока нет
- 10 AnatomyApproaches Orthobullets2017Документ177 страниц10 AnatomyApproaches Orthobullets2017jazelОценок пока нет
- Os Complete Final AnswerДокумент198 страницOs Complete Final AnswerDeshini Balasubramaniam100% (4)
- امتحان التشريح الشامل2Документ24 страницыامتحان التشريح الشامل2Muntadhar HadwanОценок пока нет
- Upper Limb 1Документ3 страницыUpper Limb 1Abdallah DarwishОценок пока нет
- UW Notes - 11 - MSK ArrangedДокумент66 страницUW Notes - 11 - MSK ArrangedDor BenayounОценок пока нет
- Edx Braquial PlexusДокумент30 страницEdx Braquial PlexusMariana GОценок пока нет